
Os Odontoideum - "MR documented Craniocervical Ligamentous Injury in Early Childhood with delayed formation of Os Odontoideum on Sequential Imaging". Case-based Review and Mini Database Analysis
Arnold H. Menezes
Department of Neurosurgery, University of Iowa Hospitals & Clinics, Iowa City, Iowa, USA
Abstract
The etiology of os odontoideum has been debated ever since its first description by Giacomini in 1886. There are proponents of congenital origin as well as reports of post-traumatic os odontoideum formation after early childhood craniovertebral junction (CVJ) trauma. We document CVJ ligamentous injury on MRI in an 18-month-old child with sequential imaging demonstrating the os odontoid formation. Our database of 260 surgically treated patients with os odontoideum was analyzed regarding etiology and associated abnormalities. The literature (1970-2022) is reviewed.
Introduction
Os odontoideum is radiographically described as an independent ossicle posterior to hypertrophic anterior atlas arch, with cortical margins, apart from a hypoplastic dens1. Ever since its first description in 1886 by Giacomini, the origin has been debated2. Numerous case reports and case series show both a possible congenital origin as well as secondary to early craniovertebral junction (CVJ) trauma3-13. There is support for both causations. We document CVJ ligamentous injury on MRI in an 18-month-old child with sequential imaging demonstrating the os odontoideum formation14. The patient also had a Chiari I abnormality on the initial MRI. He became clinically symptomatic from craniovertebral junction instability and the Chiari abnormality needing both pathologies to be addressed at age 10.
Clinical Case
In 2006 this child presented at 18 months of age after having fallen out of a crib. He was referred to University of Iowa Hospitals & Clinics because of inability to move his trunk and poor hand movement14. He did not move from side-to-side and had ecchymosis on the right forehead. A cervical collar was immediately placed, and the patient underwent magnetic resonance imaging. The cervicomedullary junction was enlarged and there was an 8-mm tonsillar herniation consistent with a Chiari I abnormality. There was an area of linear brightness on T2-W MRI lifting the anterior longitudinal ligament between C1 and C3. A small odontoid process was identified (Figure 1A, 1B). We felt that he had craniocervical ligamentous injury and cervicomedullary contusion with Chiari I abnormality. The clinical picture of neurological deficit, swollen cervicomedullary junction and MRI findings confirm the trauma to the craniovertebral area and ligamentous injury. Further evidence is the presence of bony spicule off the posterior rim of the ossiculum penetrating the dura as found at transoral resection14. He was maintained in a Philadelphia collar and started on Decadron with an immediate taper. He showed marked improvement neurologically and at 2 month follow up his neurological examination was normal.

Figure 1: A) Composite of lateral CVJ T2-W MRI. Note the prevertebral ligamentous hemorrhage (arrow) and also the cerebellar tonsillar ectopia (arrowhead). There is expansion of the cervicomedullary junction. A small odontoid process if see. B) Axial T2-W MRI at C1 level. The arrow points to the ligamentous injury.
Lateral cervical spine radiographs at 2 months showed an incomplete development of the anterior and posterior arches of the atlas with normal alignment. Magnetic resonance imaging showed soft tissue crowning of the odontoid process and cerebellar tonsillar ectopia. The prevertebral swelling had receded. The cruciate ligament and the alar ligaments were investigated as well as the tectorial membrane and found to be intact. Five months following injury his cervical spine radiographs showed no evidence of instability. An Aspen brace was maintained for a year following which a CT scan of the neck showed irregular ossification of the axis body, a hypoplastic dens on CT and a small odontoid process (Figure 2).
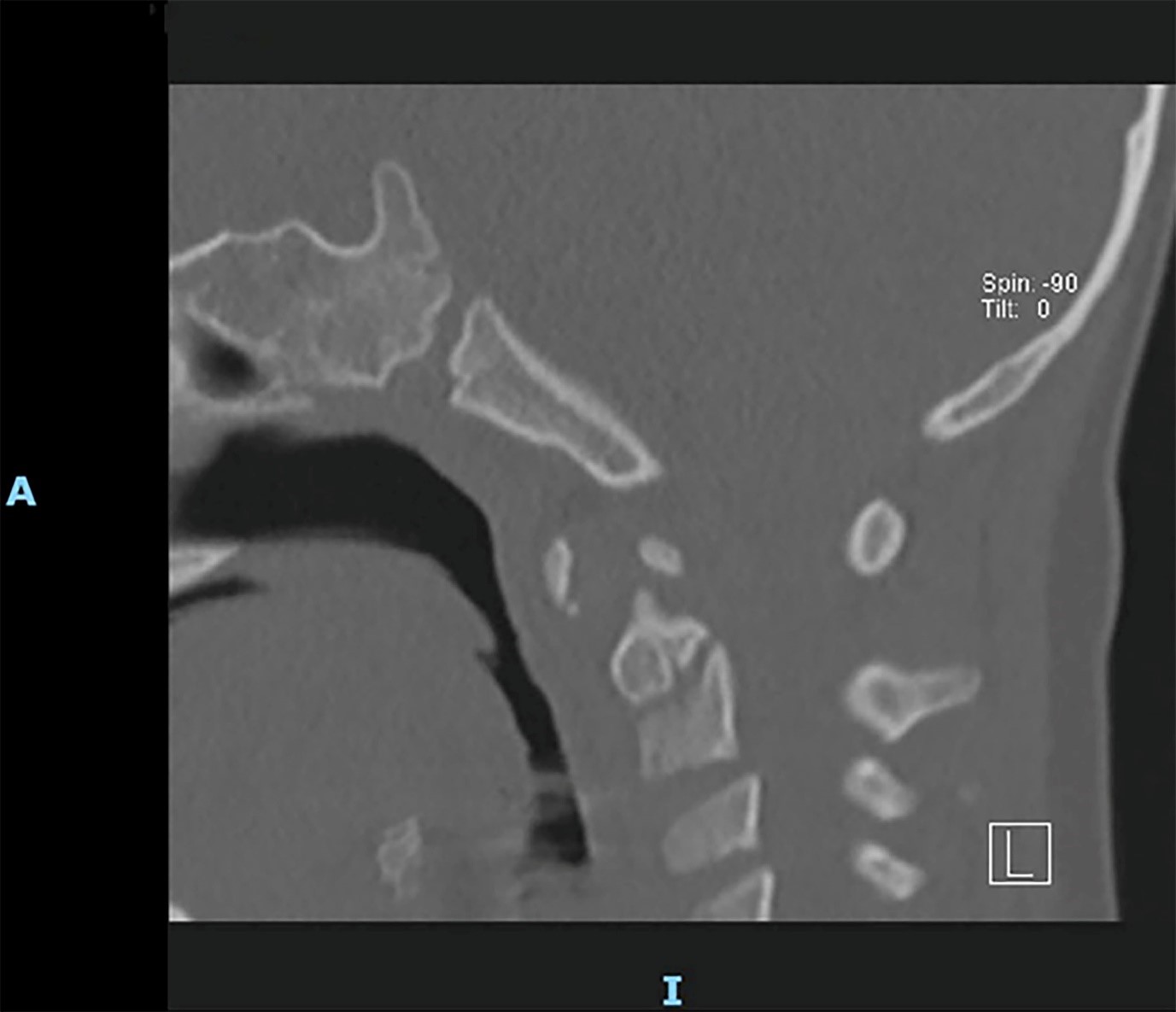
Figure 2: 2D CT of CVJ. There is a small odontoid ossicle and irregular odontoid.
At age 9 he had lateral cervical spine radiographs made elsewhere following a school altercation that demonstrated the dystopic odontoideum. He was evaluated at age 10 for neck pain and occipital headaches, difficulty swallowing and bladder incontinence. He complained of numbness in his hands and tended to drop objects. Headaches were worse with Valsalva maneuver. Magnetic resonance imaging showed the Chiari I malformation with tonsils down to 20 mm below the plane of foramen magnum and a syrinx. A large os odontoideum was visible on CT (Figure 3A, 3B). He had gross atlantoaxial instability on cervical spine dynamic radiographs. He underwent posterior fossa procedure for both the Chiari abnormality as well as dorsal occipitocervical fusion, which had to be revised. Despite this and a successful dorsal occipitocervical fusion, he had new findings of a Lhermitte’s phenomenon with neck movement a year later. This responded to an anterior transoral-transpalatopharyngeal resection of the odontoid and medullary decompression. He recovered. There was a bony spicule penetrating the dura from the posterior aspect of the os. This is only the second MRI documentation of early childhood CVJ trauma and sequential os odontoideum formation.
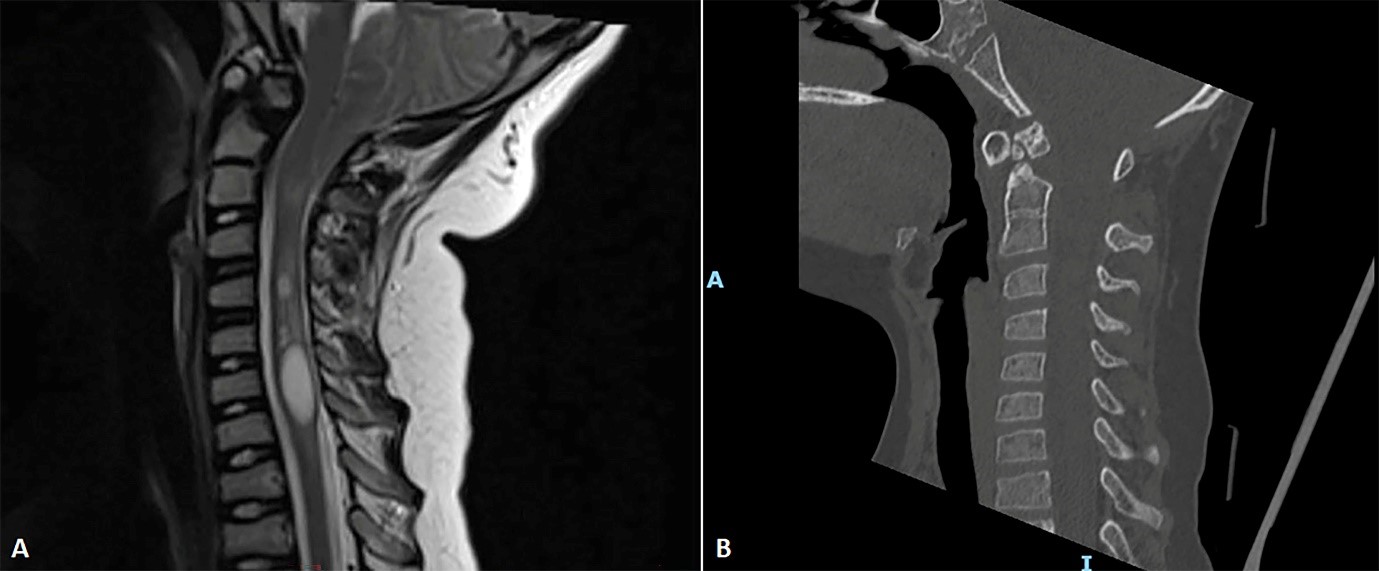
Figure 3: Composite of lateral cervical MRI (A) and 2D CT (B) made 8 years following the initial trauma. Note the os odontoideum and hypertrophic atlas anterior tubercle. The cerebellar tonsil has descended further. There is a cervical syrinx.
Database Analysis
We undertook a detailed analysis of 260 surgically treated cases of os odontoideum to document the age groups, first symptom presentation, radiographic findings and associated abnormalities to better confirm the etiology15. A literature search (1970-2022) was made to correlate our findings.
260 patients underwent surgical management of a referral database of 520 cases (1978 to 2022). All surgically treated patients underwent neurodiagnostic imaging. A history of early childhood (less than 6 years of age) CVJ trauma was investigated including obtaining emergency departments initial radiographs from the national referral and subsequent follow up. Associated radiographic and systemic abnormalities were noted. There were 156 of the 260 patients who had a previous history of early childhood trauma. We were able to obtain cervical spine documentation of a normal odontoid process at the initial injury in 54 of the 156 who subsequently developed an os odontoideum.
Discussion
The etiology of os odontoideum is debated15. Proponents of the congenital os odontoideum claim that this may be the result of failure of fusion of the odontoid apex or the main part of the odontoid or failure of separation of C1 and caudal migration. However, there is always a hypoplastic dens below the os and the gap between the two is above the lateral C1-C2 articulation and hence the etiology of failure of fusion of C1 centrum to the axis body is difficult to accept. There are reports of congenital origin with the presence of ossicle in utero images in Down syndrome16. It is also associated with syndromic abnormalities such as Morquio syndrome, Klippel-Feil syndrome, spondyloepiphyseal dysplasia, metaphyseal dysplasia, Down syndrome and other syndromes with ligamentous laxity4,11,14,15,17-19. There have been reports of familial os odontoideum as well as in twins as seen in our database as well as in the literature6-10,13,20. In our own database the ages range from 2 to 58 years. Associated abnormalities were 94/260 patients (Table 1). It appears that dystopic os odontoideum is associated with traumatic origin.
Table 1: Associated conditions with Os Odontoideum (260 patients)
|
Pathology |
# |
Age at presentation |
Orthotopic |
Dystopic |
|
Klippel-Feil syndrome* |
26 |
All ages |
9 |
17 |
|
Chiari I malformation* |
20 |
All ages |
0 |
20 |
|
Down syndrome |
11 |
2-5 years |
7 |
4 |
|
Atlas assimilation* |
8 |
2-5 years |
5 |
3 |
|
Bipartite atlas arches |
6 |
4-6 years |
0 |
6 |
|
Spondyloepiphyseal dysplasia |
6 |
6-10 years |
4 |
2 |
|
Morquio syndrome |
4 |
5-10 years |
0 |
4 |
|
Craniofacial dysostosis* |
4 |
8-10 years |
4 |
0 |
|
Spondylometaphyseal dysplasia |
2 |
< 5 years |
2 |
0 |
|
Larsen syndrome |
2 |
< 5 years |
2 |
0 |
|
Dandy-Walker malformation |
2 |
< 5 years |
2 |
0 |
|
Charge syndrome |
1 |
5 years |
1 |
0 |
|
Achondroplasia |
1 |
10 years |
0 |
1 |
|
Chondrodysplasia ossificans |
1 |
6 years |
1 |
0 |
|
TOTAL |
94 |
|
|
|
*had combination or other abnormalities
The true congenital os odontoideum has a very large ossicle and could represent a large ossiculum terminal persistens21,22. None of the post-traumatic origin had associated bony abnormalities.
Early childhood trauma was documented in our database of surgically treated cases (156/260) with a documented normal odontoid process at the first initial encounter in the emergency facilities in 54/156 with a subsequent development of os odontoideum. It was Fielding et al.3 who initially brought up the possibility of acquired post-traumatic lesion caused by odontoid injury followed by what he felt was avascular necrosis and an osseous remodeling. Zygourakis et al. in 2011 illustrated MR findings in the initial trauma of a 2-year-old child who sustained ligamentous injury and subsequent formation of os odontoideum20. It has been proposed that the initial trauma led to vascular compromise as with a type II odontoid fracture20,23,24. The apical vascular arcade23,25 continues to supply the apex of the odontoid process which enlarges as also the anterior arch of the atlas with posterior arch becoming smaller. This would be a tell-tale sign of a traumatic origin since the original cervical spine radiographs showed a normal anterior and posterior arch of the atlas. The final stage is the osseous remodeling in the development of the os odontoideum. The initial injury was likely between the upper and the lower central synchondrosis of the odontoid20,21. The associated abnormalities (94/260) in the database points also to a possible congenital origin. In our case, the increased descent of the cerebellar tonsils was likely attributed to decrease in posterior fossa volume that was corrected after resection of the os odontoideum and decompression of the medulla. Posterior craniocervical fusion has been proposed as treatment for the os odontoideum but it appears that this did not protect this child26-28.
The variants from the literature with the population base is likely due to our referral pattern and that of syndromic and pediatric population.
Acknowledgment
We acknowledge Mary Jo Piper for her assistance in formatting the paper and database.
Funding Information
This paper was supported with a gift from Sam and Betsy Reeves.
Conflict of Interest
No conflict of interest was reported by the author.
References
- Menezes AH. Congenital and acquired abnormalities of the craniovertebral junction. In: Youmans JR, ed. Neurological Surgery. WB Saunders. 1995; 1035-1089.
- Giacomini C. Sull’esistenza dell’ “os odontoideum” nell’uomo. Gior Reg Accad Med Torino. 1886; 49: 24-38.
- Fielding JW, Griffin PP. Os odontoideum: An acquired lesion. J Bone Joint Surg Am. 1974; 56A(1): 187-190.
- Fielding JW, Hensinger RN, Hawkins RJ. Os odontoideum. J Bone Joint Surg Am. 1980; 62A(3): 376-383.
- Wollin DG. The os odontoideum. J Bone Joint Surg Am. 1963; 45A(7): 1459-1471.
- Morgan MK, Onofrio BM, Bender CE. Familial os odontoideum: Case report. J Neurosurg. 1989; 70: 636-639.
- Wang S, Wang C. Familial dystopic os odontoideum: A report of three cases. J Bone Joint Surg Am. 2011; 93: e44(1-5).
- McHugh BJ, Grant RA, Zupon AB, et al. Congenital os odontoideum arising from the secondary ossification center without prior fracture. J Neurosurg Spine. 2012; 17: 594-597.
- Kirlew KA, Hathout GM, Reiter SD, et al. Os odontoideum in identical twins: Perspective on etiology. Skeletal Radiol. 1993; 22: 525-527.
- Prasad A, Shah A, Sasane S, et al. Familial os odontoideum. World Neurosurg. 2020; 141: 215-218.
- Arvin B, Fournier-Gosselin MP, Fehlings MG. Os odontoideum: Etiology and surgical management. Neurosurgery. 2010; 66: A22-A31.
- Ricciardi JE, Kaufer H, Louis DS. Acquired os odontoideum following acute ligament injury. Report of a case. J Bone Joint Surg Am. 1976; 58A: 410-412.
- Goel A, Patil A, Shah A, et al. Os odontoideum: Analysis of 190 surgically treated cases. World Neurosurg. 2020; 134: e512-e523.
- Wilson S, Menezes AH: MR documented craniocervical ligamentous injury at age 18 months: Delayed formation of os odontoideum. Complex management issues. Case-based review. Childs Nerv Syst. 2023; 39(4): 869-875.
- Menezes AH. Pathogenesis, dynamics, and management of os odontoideum. Neurosurg Focus. 1999; 6(6): article 2.
- Stevens JM, Chong K, Barber C, et al. A new appraisal of abnormalities of the odontoid process associated with atlanto-axial subluxation and neurological disability. Brain. 1994; 117: 133-148.
- McKay S, Al-Omari A, Tomlinson L, et al. Review of cervical spine anomalies in genetic syndromes. Spine. 2012; 37: E269-E277.
- Hungerford GD, Akkaraju V, Rawe SE, et al. Atlanto-occipital and atlanto-axial dislocations with spinal cord compression in Down’s syndrome: A case report and review of the literature. Br J Radiol. 1981; 54: 758-761.
- Hedequist DJ, Mo AZ. Os odontoideum in children. J Am Acad Orthop Surg. 2020; 28: e100-e107.
- Zygourakis CC, Cahill KS, Proctor MR. Delayed development of os odontoideum after traumatic cervical injury: Support for a vascular etiology. J Neurosurg Pediatrics. 2011; 7: 201-204.
- Menezes AH, VanGilder JC, Graf CJ, et al. Craniocervical abnormalities. A comprehensive surgical approach. J Neurosurg. 1980; 53: 444-455.
- Pang D, Thompson DNP. Embryology and bony malformations of the craniovertebral junction. Childs Nerv Syst. 2011; 27: 523-564.
- Schiff DC, Parke WW. The arterial supply of the odontoid process. J Bone Joint Surg Am. 1973; 55A: 1450-1456.
- Parke WW. The vascular relations of the upper cervical vertebrae. Orthop Clin North Am. 1978; 9: 879-889.
- Althoff B, Goldie IF. The arterial supply of the odontoid process of the axis. Acta Orthop Scand. 1977; 48: 622-629.
- Hadley MN, Walters BC, Grabb PA, et al. Os odontoideum. Neurosurgery. 2002; 50(3Suppl): S148-S155.
- Rozzelle CJ, Aarabi B, Dhall SS, et al. Os odontoideum. Neurosurgery. 2013; 72: 159-169.
- Klimo P Jr, Coon V, Brockmeyer D. Incidental os odontoideum: Current management strategies. Neurosurg Focus. 2011; 31(6): E10.