
The Relationship between Synovial Inflammation in Whole-Organ Magnetic Resonance Imaging Score and Traditional Chinese Medicine Syndrome Pattern of Osteoarthritis in the Knee
Gu Yu-guo, Jiang Hong*
Department of Orthopaedics and Traumatology, Suzhou TCM Hospital, in affiliation with Nanjing University of Chinese Medicine, Suzhou, China
Abstract
Purpose: The aim of this study was to guide the quantitative analysis of Traditional Chinese Medicine (TCM) syndromes by the measurement of magnetic resonance.
Methods: A total of 213 patients with knee osteoarthritis were selected for TCM dialectical classification, and their MRI images were scored on Whole-Organ Magnetic Resonance Imaging Score (WORMS) to evaluate the correlation between severity of synovitis and TCM syndrome types in the scores.
Results: Among the 213 patients, 25 were Anemofrigid-damp arthralgia syndrome (accounting for 11.7%), 84 were Pyretic arthralgia syndrome (39.4%), 43 were Blood stasis syndrome (20.2%), and 61 were Liver and kidney vitality deficiency syndrome (28.6%). In the WORMS score, 12 (5.6%) had a synovitis score of 0, 60 (28.2%) had a synovitis score of 1, 50 (23.5%) had a synovitis score of 2, and 91 (42.7%) had a synovitis score of 3. There was a statistically significant difference in the correlation analysis. The group with a synovitis score of 3 in WORMS was more likely to occur in the Pyretic arthralgia syndrome (X2 = 194.424, P = 0.000).
Conclusion: In this study, Pyretic arthralgia syndrome (39.4%) was found to be the main clinical manifestation in patients with knee osteoarthritis synovitis. This finding has certain guiding significance for relevant treatment.
Introduction
Traditional Chinese medicine (TCM) is an ancient and still very vital holistic system of health and healing, based on the notion of harmony and balance also employing the ideas of moderation and prevention. The philosophies and principles of traditional Chinese medicine explain how the body works as an integrated system. The concepts of Chinese medicine closely parallel the theories that Western medicine is now discovering. For example, there is an understanding that the acupuncture meridians are channels of communication that follow the fascia; the systems theory supports the principle of the body as a networked system. Chinese medicine recognizes that the accumulation and balance of the attributes within an individual (Yin–Yang, heat–cold, blood–Qi) determines their internal climate, and therefore their health or disease.
Osteoarthritis (OA) is defined as a disease which involves an entire joint. It not only affects the cartilage but also the structures and metabolic changes of subchondral bone and synovial tissue1,2. Various reports have shown that synovitis is a key factor which associates with OA pain and symptoms, and even occurs in the early phase of osteoarthritis3-5. New imaging technologies (ultrasonic imaging and magnetic resonance imaging) have proven that 70% of patients with osteoarthritis are infected by both OA and synovitis, 95% of which presents synovitis accompanied by hydrarthrosis6.
Synovial inflammation is a process characterized by synovial thickening (hypertrophy and hyperplasia) and cellular infiltration (of lymphocytes and macrophages)7,8. The histological analysis of OA-infected synovium presented an increase of synovial lining cells and infiltrating cells in number, of which the majority were macrophages7,9 while only an extremely small proportion were B and T cells10. The symptom of synovitis has been now recognized as a key characteristic of OA symptoms and progression11.
Traditionally, osteoarthritis (OA) is categorized within non-inflammatory arthritis. However, with increased understanding of the persistent immune response process of OA-infected joints and synovium, the differentiation between inflammatory arthritis and degenerative arthritis becomes more and more blurred. Synovitis is defined as synovial inflammation, which is a characteristic of classic inflammatory arthritis. Increasingly, scholars are becoming aware of the fact that a considerable part of patients with primary OA show synovitis. In light of this observation, further research has found the presence of arthritis and synovitis in the pathogenesis of OA.
Knee osteoarthritis with synovitis is categorized in “knee paralysis diseases” in traditional Chinese medicine. It develops from degenerative changes of articular cartilage, with synovial injury of articular capsule, synovial hyperemia, and inflammatory exudation as its major pathological changes. In clinical, degenerative osteoarthropathy with swelling, pain and difficult extension and flexion of the knee joint (as the main manifestations) is most often diagnosed in middle-aged and elderly people.
In modern medicine, phlegm is the thick viscous substance secreted by the mucous membranes of the respiratory passages but in traditional Chinese medicine, the cause of phlegm is a special concept caused by a special kind of pathogenic factors. It is different from wind, cold, heat, dampness, dryness and fire, the pathogenic factors. It is also different from seven emotions, diet, overwork internal injuries pathogenic factors, but also is closely related to the etiology.
It is formed by these pathogenic factors acting on the human body after a pathological product. Deng Jinfeng12 considers the root cause of the disease to be the deficiency of liver and kidney as well as the motor impairment syndrome of the knee joint, which is manifested as obstruction syndrome of bone and joint. The disease is characterized with “motor impairment as the root cause and rheumatism as the symptom”. Similarly, He Xian13 suggested the root cause to be liver and kidney deficiency and the symptoms to be the stagnation of vital energy circulation, blood stasis and phlegm coagulation, the invading and attacking of wind-cold damp pathogen, as well as the obstruction of main and collateral channels.
To summarize the ideas above, most of these skilled doctors agree that knee osteoarthritis with synovitis is fundamentally caused by gradual deficiency of liver and kidneys, insufficiency of vital energy and blood, and dystrophy of muscles and bones. The pain is stimulated by loss of the five key elements and dystrophy of internal organs and meridians. In addition, wind-cold damp pathogens attack joints at the weak point, or falling occurs which results in joint spraining, or long-term strain takes place on joints, all leading to obstruction of main and collateral channels, blood stasis, stagnation of bone arteries and veins, while obstruction triggers pain.
The TCM syndrome differentiation was conducted by reference to the Diagnosis and Treatment of Knee Paralysis Disease (Knee Osteoarthritis) by ‘the 11th Five-Year Plan’ Key Specialty Cooperative Team of the State Administration of Traditional Chinese Medicine14. Thus, knee osteoarthritis was differentiated into four syndrome types:
(1). Anemofrigid-damp arthralgia syndrome: the knee joint presents the feeling of heaviness, souring and pain, or swelling, and even difficulty in extension and flexion. The painful sites are more stationary, but sometimes migrate. The symptoms are intensified during cold or rainy days. The skin does not turn red or hot; the tongue presents a layer of thin and white fur; and the pulse is wiry and tense.
(2). Pyretic arthralgia syndrome: the knee joint shows pain, redness and hotness, with severe swelling and pain. If treated with cold therapy, the knee joint becomes less painful. The muscles and vessels around the area are spastic. The symptoms are mild during day-time hours but severe at night, accompanied with fever, thirst, worrying, restlessness, red tongue, slimy yellow fur or dried yellow fur on the tongue, as well as a rolling and rapid pulse pattern.
(3). Blood stasis syndrome: the knee joint is in pain and sensitive to pressure when pressed on, present’s uncomfortable swelling and can be described as being as painful as being stabbed by an awl or other sharp pointy objects. The symptoms are mild during the day but turn severe at night or can persist without showing signs of relief. The joint has difficulty with motion, preventing internal or external rotation. Patients in this TCM syndrome type often exhibit a darker complexion and whitening of the lips. Their tongues turn green or grow ecchymosis. Their pulses are more are tense and erratic, or thread and rapid. The course of disease is persistent, and the knee joint often shows injuries and a history of strain.
(4). Liver and kidney vitality deficiency syndrome: the diseased knee and leg both ache and limp, or are in persistent pain. The syndrome type is usually accompanied by pain in the waist and lower extremities, and the diseased parts require pressing and rubbing to alleviate the symptoms. If used excessively or to the point of exhaustion, the diseased knee will deteriorate. Lying down is a way to mitigate the discomfort, but the symptoms re-occur frequently. The pulse pattern of this syndrome type is deep and thread-like, or deep and forceless.
This study conducted a preliminary discussion on the correlation between the imageology and TCM syndrome types of knee osteoarthritis with synovitis.
Data and Methods
General Data
With an incomplete random sampling from patients with knee osteoarthritis and receiving knee joint X-ray and MRI examinations at the outpatient facility of orthopedics and traumatology department, Suzhou Hospital of Traditional Chinese Medicine, from January 2015 to June 2018, 213 patients (32 men and 181 women) were selected and given follow-ups, with an average age of 65.8±7.78 years old and a preoperative history of joint pain for 1 month to 10 years.
Inclusion criteria: 1. patients who were older than 40 years old; 2. patients who met the OA diagnostic criteria from the diagnostic criteria of knee osteoarthritis in Chinese Osteoarthritis Diagnosis and Treatment Guideline (2007)15. That is, (1). the patients should suffer repeated knee joint pain in the past month; (2). their X-ray images (in standing or weight-bearing position) prompted narrowing of knee joint space, subchondral sclerosis and (or) cystic degeneration, and forming of osteophyte on the margin of knee joint; (3). their synovial fluid (at least twice) was clear and thick, and WBC<2000 cells/ml; (4). the middle-aged and elderly patients ≥40 years old; (5). patients suffering morning stiffness ≤30min; (6). patients presenting bony crepitus (sense of friction) when moving the knee joint. Patients who met conditions (1)+(2), or (1)+(3)+(5)+(6), or (1)+(4)+(5)+(6), can be diagnosed with knee OA. 3. Patients with a course of disease longer than 1 month; 4. patients with an X-ray evaluation: K/L level ≥ level 2. In the light of Kellgren’s and Lawrence’s diagnostic criteria of radiology16, osteoarthritis was graded into 5 levels, where level 0 meant normal joint; level I prompted suspected narrowing of joint space and possible presence of osteophytes; level II prompted obvious presence of osteophytes and suspected narrowing of joint space; level III prompted a middle volume of osteophytes, relatively apparent narrowing of joint space, and the presence of sclerotic changes; level IV prompted a large volume of osteophytes, significant narrowing of joint space, and severe sclerotic lesions and explicit deformities. 5. Patients whose MRI images specified OA accompanied by synovitis/synovial fluid. Referring to the synovitis scoring in WORMS score, the specific criteria of scoring is as follows. Though there was no differentiation between synovium thickening and hydrarthrosis, the estimated maximum expansion of the synovial cavity enabled overall scoring from 0 to 3 points. Score 0 meant normal joint; score 1 meant an expansion smaller than 33% of the maximum potential expansion; score 2 meant an expansion which was 33%-66% of the maximum potential expansion; and score 3 meant an expansion larger than 66% of the maximum potential expansion17.
Exclusion criteria: (1) patients with injuries of knee, broken skin and cutaneous ulcer, or with a history of surgery or knee injection; (2) patients with immunological diseases and immune associated arthritis, such as rheumatoid arthritis, ankylosing spondylitis, reactive arthritis, psoriatic arthritis, and Reiter’s syndrome, or with renal insufficiency in need of blood dialysis or peritoneal dialysis, or with a history of cancer (except for non-melanoma skin cancer), and so forth; (3) patients who had recently received a treatment with systemic corticosteroid, injection of intraarticular drugs, and treatments with other relevant drugs; (4) patients with contradicting MRI examinations who were unable to cooperate and complete examinations, as well as those whose scanning images did not meet the diagnostic criteria.
TCM Syndrome Differentiation and Auxiliary Examinations
Each case was differentiated by TCM syndromes and completed X-ray and MRI examinations. The MRI images of the disease were evaluated by a WORMS score17, and the WORMS score system is shown in Table 1. Two radiologists, who had engaged in joint imaging diagnosis for over 5 years and 10 years, respectively, were hired to read the images and measure, without given any patient information, clinical history and previous image data. The final values were means of the measurements the two radiologists obtained.
Table 1: WORMS score table
|
Part |
Medial tibiofemoral joint |
Lateral tibiofemoral joint |
Patellofemoral joint |
S zone |
Total count |
|
1.Cartilage |
30 |
30 |
24 |
|
84 |
|
2.Marrow abnormality |
15 |
15 |
12 |
3 |
45 |
|
3.Bone cysts |
15 |
15 |
12 |
3 |
45 |
|
4.Bone attrition |
15 |
15 |
12 |
|
42 |
|
5.Osteophytes |
35 |
35 |
28 |
|
98 |
|
6.Compartment total |
110 |
110 |
88 |
|
|
|
7.Menisci |
6 |
6 |
|
|
12 |
|
8.Ligaments |
|
|
|
|
3 |
|
9.Synovitis |
|
|
|
|
3 |
|
Total |
|
|
|
|
332 |
Note: The data shown in the Table is the highest score of each part. 0 represents the normal joint.
Statistical analysis
SPSS 21.0 statistical software was used. Qualitative data using (x-bar±s) suggested adopting one-way ANOVA for multi-inter-group comparisons; enumeration data using n(%) suggested using Chi-square analysis for inter-group comparisons; and testing benchmark p<0.05 represented the difference of statistical significance.
Results
A total of 213 patients, who were qualified to both inclusion criteria and exclusion criteria, and had completed and held proper MRI images, were finally collected in the study, with an age range of 44-84 years old and averaged at 65.8±7.78 years old; 181 men and 32 women. The sample included 90 left knees and 123 right knees; in terms of TCM syndrome types, 11.7% (25/213) of the patients were diagnosed with wind cold dampness arthralgia type, 39.4% (84/213) with wind dampness heat arthralgia type, 20.2% (43/213) with blood stasis and obstruction type, and 28.6% (61/213) with liver and kidney deficiency syndrome, as shown in Table 2.
Table 2: Description and statistics of basic data
|
Indicator |
Count |
Percentage |
|
|
Gender |
Male |
32 |
15 |
|
Female |
181 |
85 |
|
|
Limb |
Right knee |
123 |
57.7 |
|
Left knee |
90 |
42.3 |
|
|
Dialectical classification |
Anemofrigid-damp arthralgia syndrome |
25 |
11.7 |
|
Pyretic arthralgia syndrome |
84 |
39.4 |
|
|
Blood stasis syndrome |
43 |
20.2 |
|
|
Liver and kidney vitality deficiency syndrome |
61 |
28.6 |
|
|
K&L type |
Type 3 |
117 |
54.9 |
|
Type 4 |
96 |
45.1 |
|
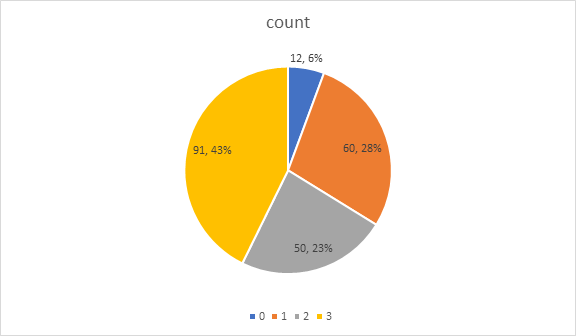
Pie chart Distribution of synovitis
As shown in the pie chart, there were 91 cases (43%) with synovitis score of 3, 50 cases (23%) with synovitis score of 2, 60 cases (28%) with synovitis score of 1, and 12 cases (6%) with synovitis score of 0. Therefore, in the patients of knee osteoarthritis, the synovial membrane has obvious inflammation of the majority of patients.
According to the Table 3, the comparison of TCM syndromes between synovitis with different severity and WORMS scores demonstrates a difference of statistical significance (Chi-square=137.286, P=0.000); the groups with a synovitis score of 0, 1 and 2 points are more vulnerable to the syndrome of deficiency of liver and kidney, while the group with a synovitis score of 3 points are more prone to the syndrome of wind dampness heat arthralgia.
Table 3: Relationship between severity of synovitis and TCM syndromes
|
|
Anemofrigid-damp arthralgia syndrome |
Pyretic arthralgia syndrome |
Liver and kidney vitality deficiency syndrome |
Blood stasis syndrome |
Chi-square |
P |
|
|
Synovitis score |
0 |
2(16.7%) |
0(0) |
8(66.7%) |
2(16.7%) |
137.286 |
0.000 |
|
1 |
12(20%) |
0(0) |
28(46.7%) |
20(33.3%) |
|||
|
2 |
10(20%) |
4(8%) |
19(38%) |
17(34%) |
|||
|
3 |
1(1.1%) |
80(87.9%) |
6(6.6%) |
4(4.4%) |
|||
Note: Kruskal-wallis test was used for comparison.
Discussion
The regional characteristics are obvious, and the sample size is small, which is also our current research deficiencies. We assisted by imaging data of clinical diagnosis, as a new viewpoint of knee joint osteoarthritis, and to observe the index quantification, this for our future clinical diagnosis and treatment of instruction, there is a new on subsequent syndrome differentiation of traditional Chinese medicine treatment also have a reference, if have the opportunity to further breakthroughs in technology, later we will use the enhanced magnetic resonance imaging (MRI), measure the synovial membrane and the volume of fluid, further on the data of quantitative synovitis. This is also our future development direction.
Knee osteoarthritis in Pyretic arthralgia syndrome, their MRI images, articular cavity has obvious effusion (87.9%), and even accompanied by a large number of effusion, synovial usually have obvious hyperplasia, past experience in clinical work, we found that the synovial inflammation is author (MRI showed obvious effusion), generally accompanied by obvious joint swelling, fever, floating patellar test is positive. Extract the tongue coating pulse phase of this kind of patients, more in line with the "Pyretic arthralgia syndrome" performance.
Traditional Chinese medicine (TCM) holds that syndrome is a pathological generalization of the disease location, etiology, disease nature and disease situation at a certain stage in the process of disease. The syndrome is a combination of the pathogenic factors and the body reaction, and a conclusion about the current nature of the disease. However, the dialectical basis of TCM often comes from personal cognition. Sometimes, different doctors may identify different syndrome types for the same patient. In order to increase the objective basis, MRI imaging can be used as a lateral reference. In our study, we found that rheumatic fever and arthralgia syndrome was predominant in knee osteoarthritis(KOA) patients. This patient is associated on MRI with marked synovitis. Therefore, we can verify our clinical diagnosis of rheumatic fever syndrome type by MRI findings of synovitis. In addition, for the other three syndrome types, the synovial inflammatory response was significantly lower on MRI.
The regional characteristics are obvious, and the sample size is small, which is also our current research deficiency. We assisted by imaging data of clinical diagnosis, as a new viewpoint of knee joint osteoarthritis, and to observe the index quantification, this for our future clinical diagnosis and treatment of instruction, there is a new on subsequent syndrome differentiation of traditional Chinese medicine treatment also have a reference, if have the opportunity to further breakthroughs in technology, later we will use the enhanced magnetic resonance imaging (MRI), measure the synovial membrane and the volume of fluid, further on the data of quantitative synovitis. This is also our future development direction.
References
- Loeser RF, Goldring SR, Scanzello CR, et al. Osteoarthritis: a disease of the joint as an organ. Arthritis Rheum. 2012; 64(6): 1697-1707.
- Krasnokutsky S, Attur M, Palmer G, et al. Current concepts in the pathogenesis of osteoarthritis. Osteoarthritis Cartilage. 2008; 16 Suppl 3: S1-3.
- Scanzello CR, Goldring SR. The role of synovitis in osteoarthritis pathogenesis. Bone. 2012; 51(2): 249-257.
- Sellam J, Berenbaum F. The role of synovitis in pathophysiology and clinical symptoms of osteoarthritis. Nature Reviews Rheumatology. 2010; 6(11): 625-635.
- De Lange-Brokaar BJ, Ioan-Facsinay A, van Osch GJ, et al. Synovial inflammation, immune cells and their cytokines in osteoarthritis: a review. Osteoarthritis Cartilage. 2012; 20(12): 1484-1499.
- Henrotin Y, Lambert C, Richette P. Importance of synovitis in osteoarthritis: evidence for the use of glycosaminoglycans against synovial inflammation. Seminars in Arthritis and Rheumatism. 2014; 43(5): 579-587.
- Benito MJ, Veale DJ, FitzGerald O, et al. Synovial tissue inflammation in early and late osteoarthritis. Annals of the Rheumatic Diseases. 2005; 64(9): 1263-1267.
- Goldenberg DL, Egan MS, Cohen AS. Inflammatory synovitis in degenerative joint disease. The Journal of Rheumatology. 1982; 9(2): 204-209.
- Farahat MN, Yanni G, Poston R, et al. Cytokine expression in synovial membranes of patients with rheumatoid arthritis and osteoarthritis. Annals of the Rheumatic Diseases. 1993; 52(12): 870-875.
- Bondeson J, Foxwell B, Brennan F, et al. Defining therapeutic targets by using adenovirus: blocking NF-kappaB inhibits both inflammatory and destructive mechanisms in rheumatoid synovium but spares anti-inflammatory mediators. Proceedings of the National Academy of Sciences of the United States of America. 1999; 96(10): 5668-5673.
- Felson DT. Clinical practice. Osteoarthritis of the knee. The New England Journal of Medicine. 2006; 354(8): 841-848.
- Jinfeng D, Guangling Z, Jinwen L. Clinical diagnosis and treatment of special diseases in orthopedics and traumatology. 2005; 282-289.
- Xian H, Chunshan W, Zhigang C, et al. Study on pathogenesis, prevention and treatment of knee osteoarthritis in TCM. Shandong Journal of Traditional Chinese Medicine. 2005; 02: 73-75.
- State administration of traditional Chinese medicine “Eleventh five-year plan" key specialist cooperation group. Diagnosis and treatment plan of the knee paralysis disease (Knee osteoarthritis) Beijing: People's medical publishing house; 2009; 18-19.
- Branch CMABS. Guidelines for the Diagnosis and treatment of osteoarthritis (2007 edition). Chinese Journal of Orthopaedic Surgery. 2007; 27: 793-796.
- Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Annals of the Rheumatic Diseases. 1957; 16(4): 494-502.
- Peterfy CG, Guermazi A, Zaim S, et al. Whole-Organ Magnetic Resonance Imaging Score (WORMS) of the knee in osteoarthritis. Osteoarthritis Cartilage. 2004; 12(3): 177-190.