
No-touch smartphone technique to confirm acetabular cup position in Total Hip Replacement
Adeel Hamid*, Usman Gill, Mian Hanif
Department of Orthopaedic Surgery, Lahore General Hospital and Post Graduate Medical Institute, Lahore, Pakistan
Abstract
In order to achieve good results following Total hip replacement , proper and reproducible acetabular cup placement is of paramount importance. The safe zone described by Lewwinick is still considered to be the target cup position. Various techniques have been used to improve the precision and accuracy of cup placement including the use of computer navigation which is often prohibitively expensive for developing countries. We present a ‘No touch smartphone technique’ to check positioning of acetabular cup intra operatively, without compromising the sterility of the operative field which we have found to be simple, quick, inexpensive and reproducible.
Introduction
With increasing numbers of Total hip replacement procedures being performed around the world it is important to improve results and minimize complications. One of the most important considerations during the surgical procedure is proper component positioning especially that of the acetabular cup1,2,3,14. This not only improves the biomechanics of the prosthetic joint but also minimizes wear and the chances of peri-operative dislocation2,4.
Despite some reservations the safe zone described by Lewwinick et al. (inclination of 40 +/- 10 and anteversion of 15 +/- 10) is still considered to be the target that most surgeons aim to achieve3,4,14. Various techniques and instruments have been used by surgeons to achieve this target. Free hand technique has yielded inconsistent results when trying to place the acetabular component in this safe zone5,7,16. This has led to the use of technology per-operatively to improve positioning6. Use of computer assisted navigation or hand held navigation systems is the norm in developed countries with no dearth of time or funds. However, the cost and time required to incorporate such technology is almost prohibitive in developing countries.
Smartphones are owned and carried by almost everyone including doctors and paramedical staff15. Various techniques have been reported using smart phones to guide cup placement. However, all of them require the surgeon to come in physical contact with the phone which can be tedious and most importantly can violate the sterile operative field8,9,10.
We describe a ‘No-touch smartphone technique’ without the surgeon having to hold the device which we found to be easy to use, quick, and reproducible.
Technique
Written informed consent was taken by all patients as the technique involved taking pictures of the operative field. The camera function of iPhone X (IOS 14.3) was used along with the markup function in photo editor.
The patient was placed in lateral decubitus position using simple posterior support for lumbar spine and anterior support for the ASIS to prevent pelvic movement. Operating table was kept horizontal using the table adjustment controls and this was re-checked before starting the procedure using a spirit level. A reference line parallel to the floor (a hence a true horizontal) was marked on the opposite wall using a spirit level, Line A-this line will be used for measuring the inclination angle.
After painting and draping direct lateral approach or posterior approach was used for all cases depending of the preference of the operating surgeons. Most cases were performed by fellows or junior consultants. During preparation of the acetabulum, anatomical landmarks, particularly the transverse acetabular ligament was used to guide reaming. After reaming was complete and when the acetabular component was being placed, 2 pictures were taken using the iPhone X by an unscrubbed member of the operating team. The first picture was taken from the dorsal aspect of the patient as shown in Figure 1. This picture was then edited as explained in Figures 3, 4 and 5. The picture was rotated using crop function to make Line A horizontal and hence at 0 degrees. Line B was drawn along the acetabular cup impactor handle. Angle between lines A and B can be directly measured and would depict the inclination angle on the cup.
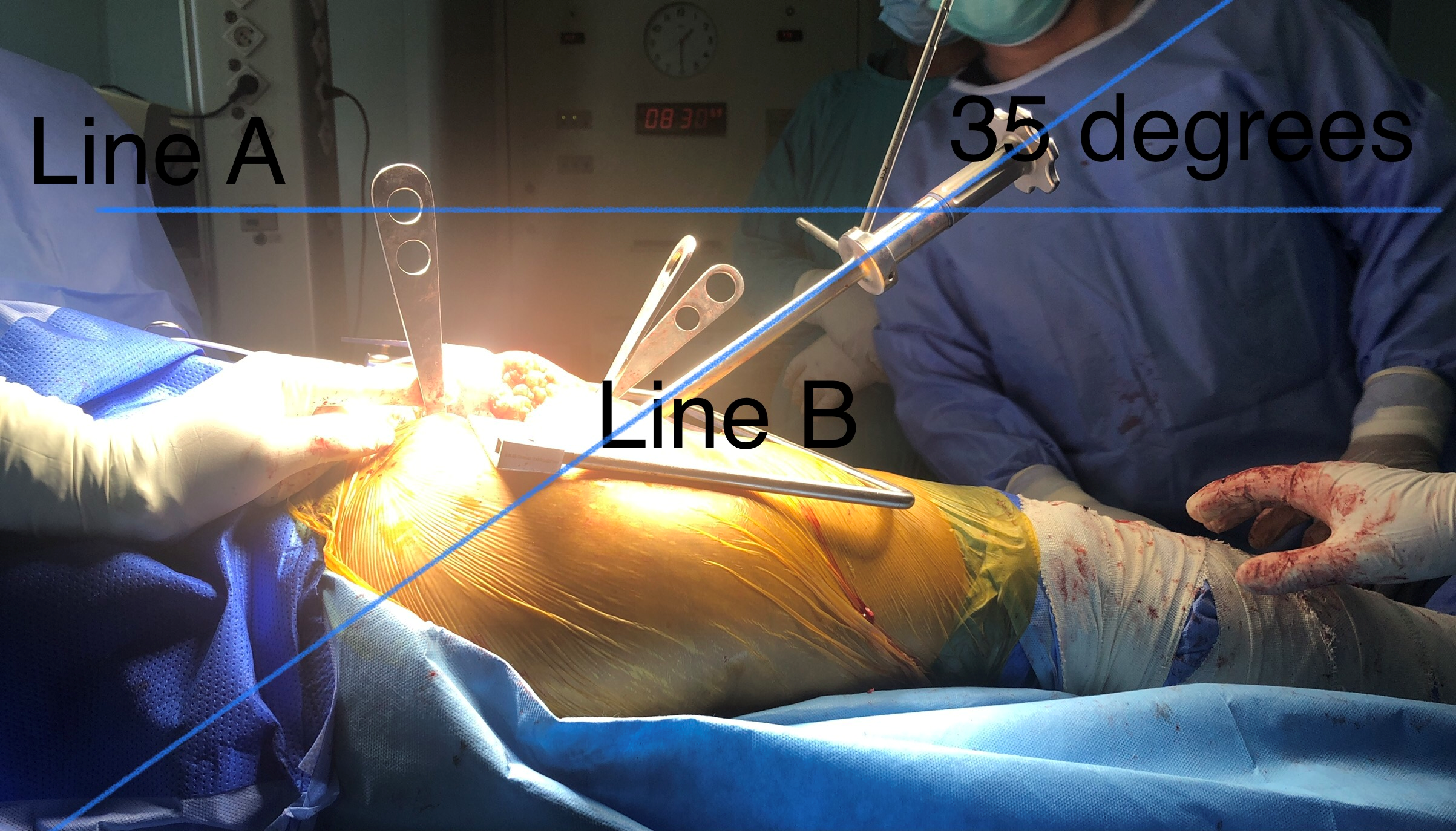
Figure 1: First picture to measure cup inclination (details in the text). The reference line A has been made parallel to the floor and hence horizontal using crop function in photo editor. Line B is drawn along the acetabular cup insertion handle. Angle between lines A and B is the cup inclination angle.
The second picture was taken from the top (Figure 2). A midaxillary line was marked on the patient’s torso pre-operatively to denote the coronal plane, Line C (this will be used as reference to measure anteversion angle). Another line was drawn along the cup impactor handle again using the markup function in photo editor, Line D. The picture was rotated with the crop function to make Line C horizontal and hence at 0 degrees. Now angle between the two lines can directly be measured. The angle between lines C and D was taken as the anteversion angle.
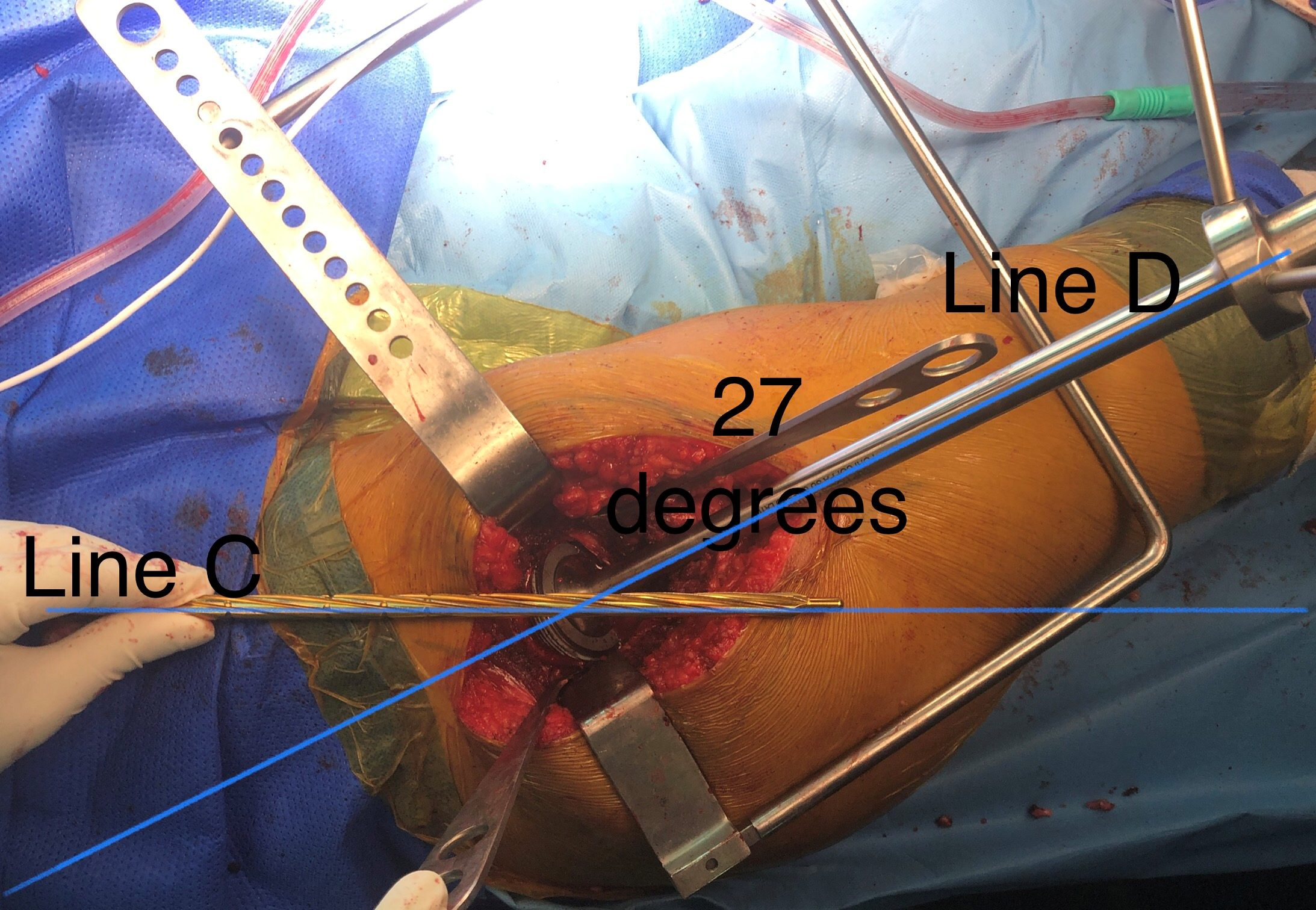
Figure 2: Picture taken from the top to measure anteversion of the acetabular cup. In this case the midaxillary line (line C) represents coronal plane and will be used as reference to measure anteversion angle. Angle between lines C and D is cup anteversion.
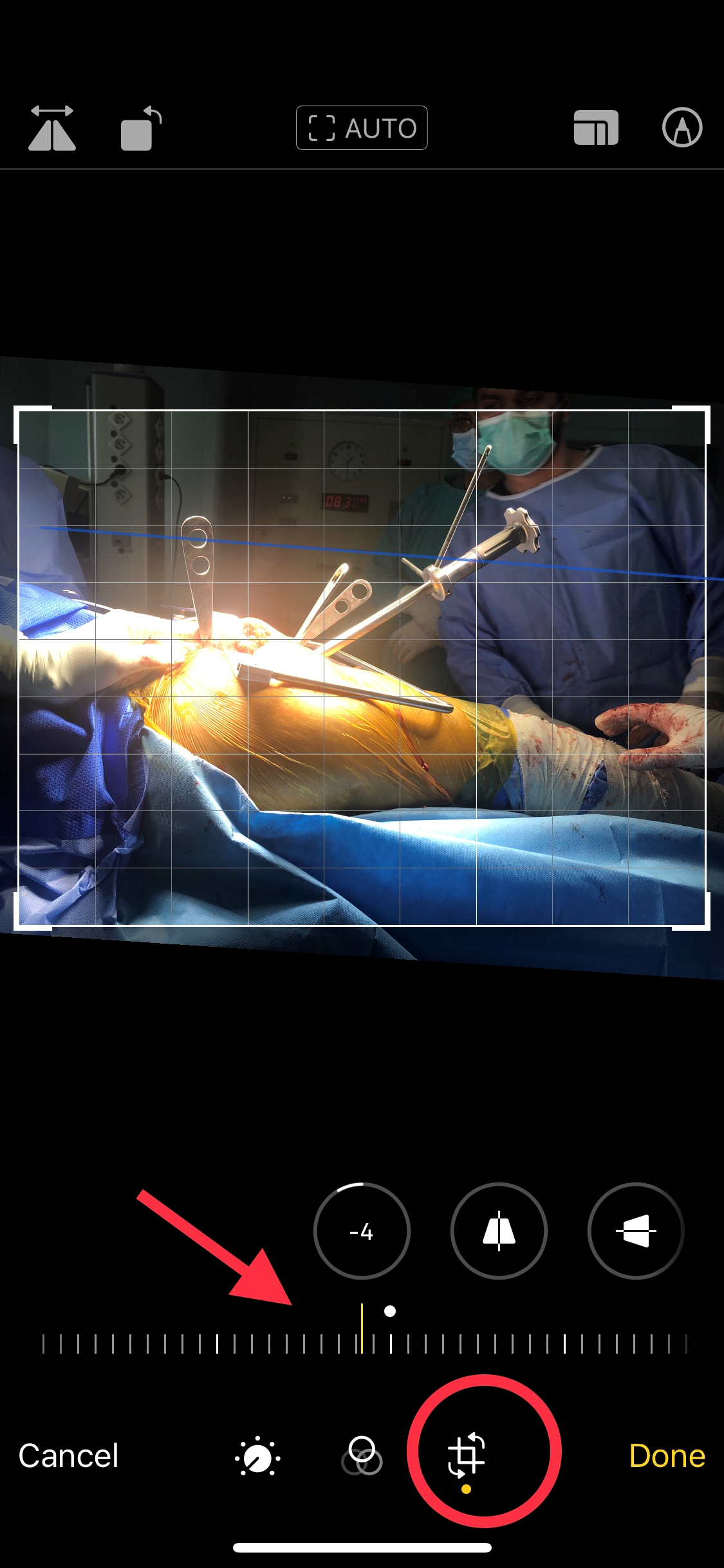
Figure 3: Using the photo editor function of Iphone X no additional app is required. Crop function (circled in red) is selected in photo editor. The picture is rotated (red arrow) till the blue reference line (marked on the opposite wall) is parallel to the grid lines (white) this ensures that that the reference line is horizontal i.e., at 0 degrees. Making the reference line horizontal makes it easier to measure the angle.

Figure 4: The markup function (red circle) and ruler (red arrow) are used to draw a line along the acetabular insertion handle. The ruler function can be used to draw lines and measure angles.
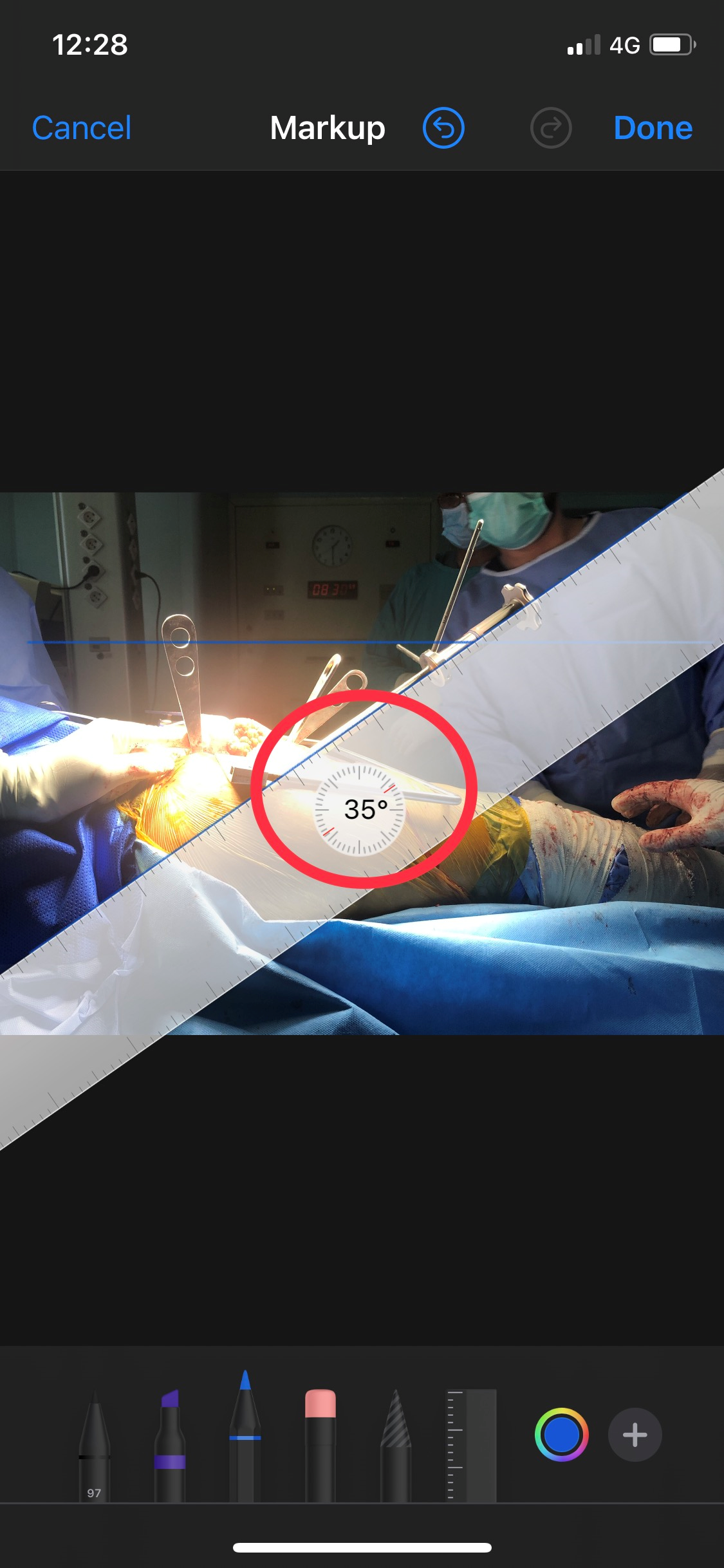
Figure 5: The same ruler function can used to directly measure the angle between the acetabular insertion handle and the reference line.(which is now parallel to the floor and hence a true horizontal). Now angle can be measured directly- placing two fingers on the ruler will show the angle.
Post operative Xray pelvis AP view with both hips was used to draw and measure the angle of inclination of the acetabular cup, taking the trans-ischeal line as horizontal. Second line was drawn tangential to the face of the acetabular cup. The angle between these two lines was the radiological inclination angle (Figure 6).
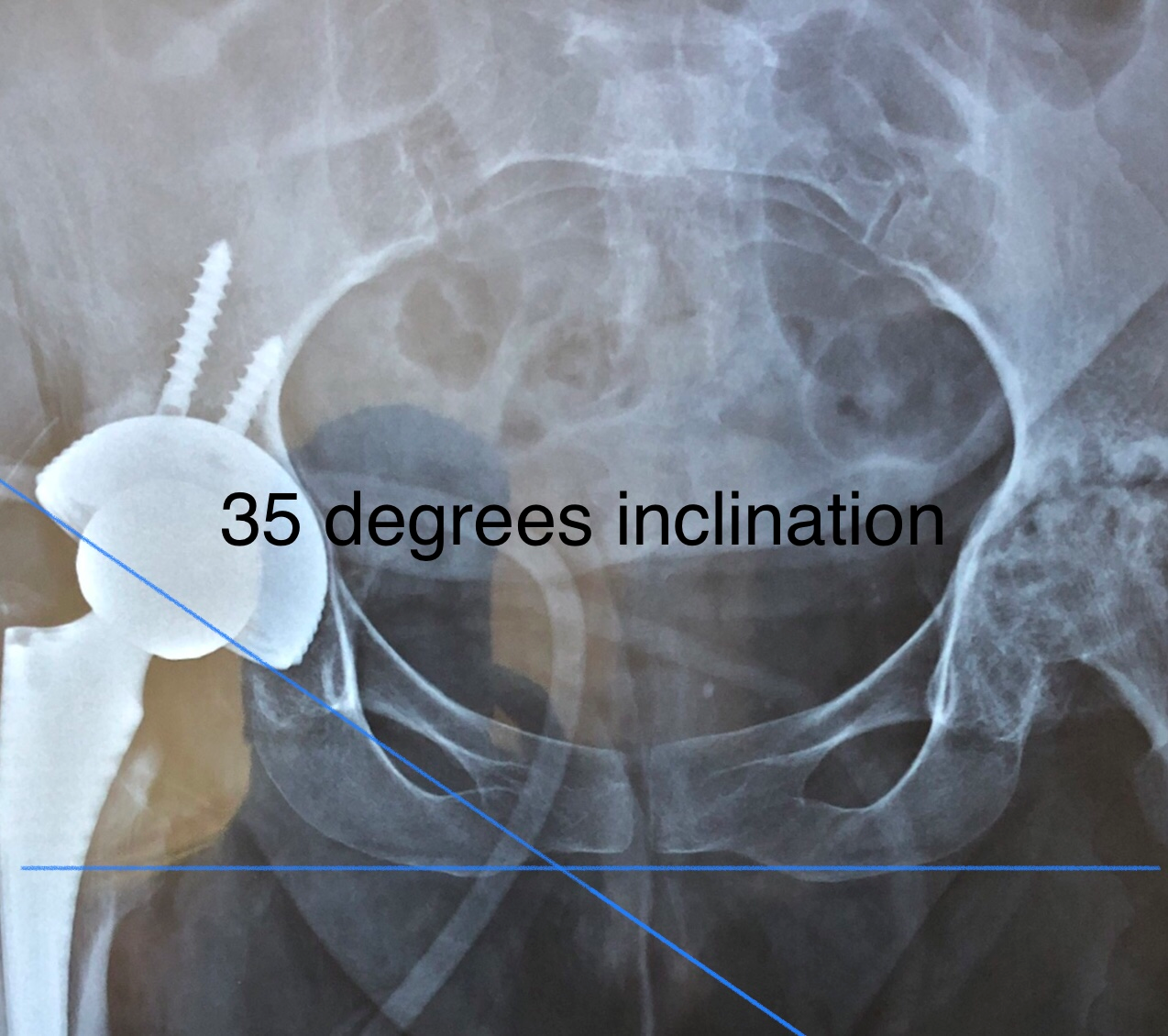
Figure 6: Post operative radiograph showing radiological cup inclination.
It has been suggested in various studies that even with ideal positioning of cross table lateral radiographs CT scan remains more accurate in measuring cup anteversion17. Hence, CT scans were used to measure the anteversion angle (reported by Consultant radiologist of our institute). First, the position of the acetabulum was standardized for rotation and pelvic tilt by reformatting the image to make the plane defined by the posterior border of distal sacrum and posterior border of ischium horizontal. Second, a plane orthogonal to the line drawn from the most medial to most lateral parts of the cup is created. Images in this plane allow for the measurement of cup anteversion (Figure 7).
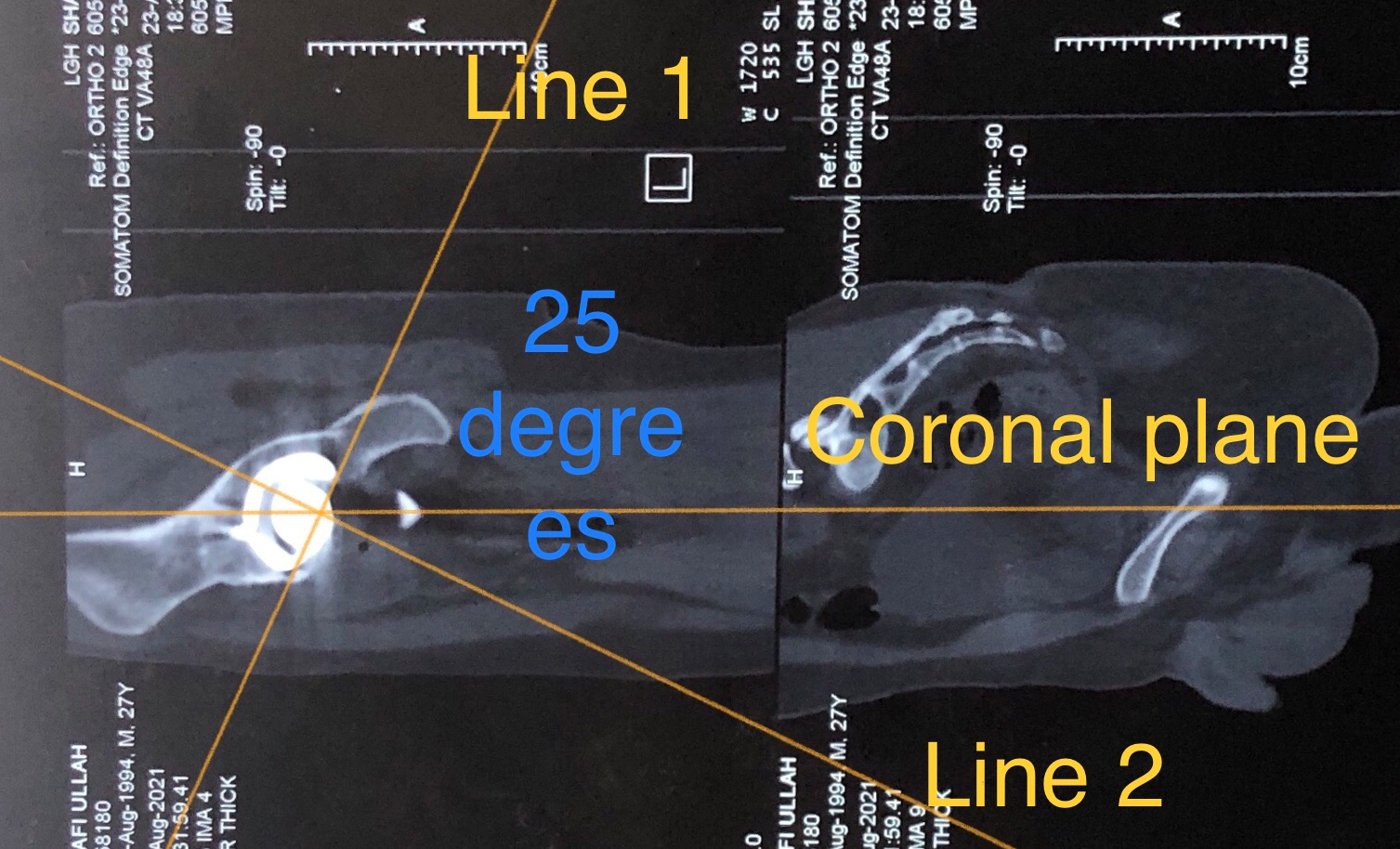
Figure 7: Post operative CT scan showing radiographic cup anteversion (as reported by Radiologist). Line 1 joins the medial and lateral parts of the cup. Line 2 is perpendicular to line 1. Angle between line 2 and coronal plane is the anteversion.
If the per operative angles measured by our technique matched the post operative radiological angles for cup positioning, we took it as evidence of the technique’s accuracy.
Results
This study was carried out in Lahore General Hospital and Post Graduate Medical Institute, Pakistan from March 2021 to September 2021. 20 patients were included in the study, 12 were male and 8 female. Ages ranged from 37 to 81 years (average age 55.3 years). Diagnoses included primary hip osteoarthritis, AVN, post traumatic arthritis and neglected hip dislocation.
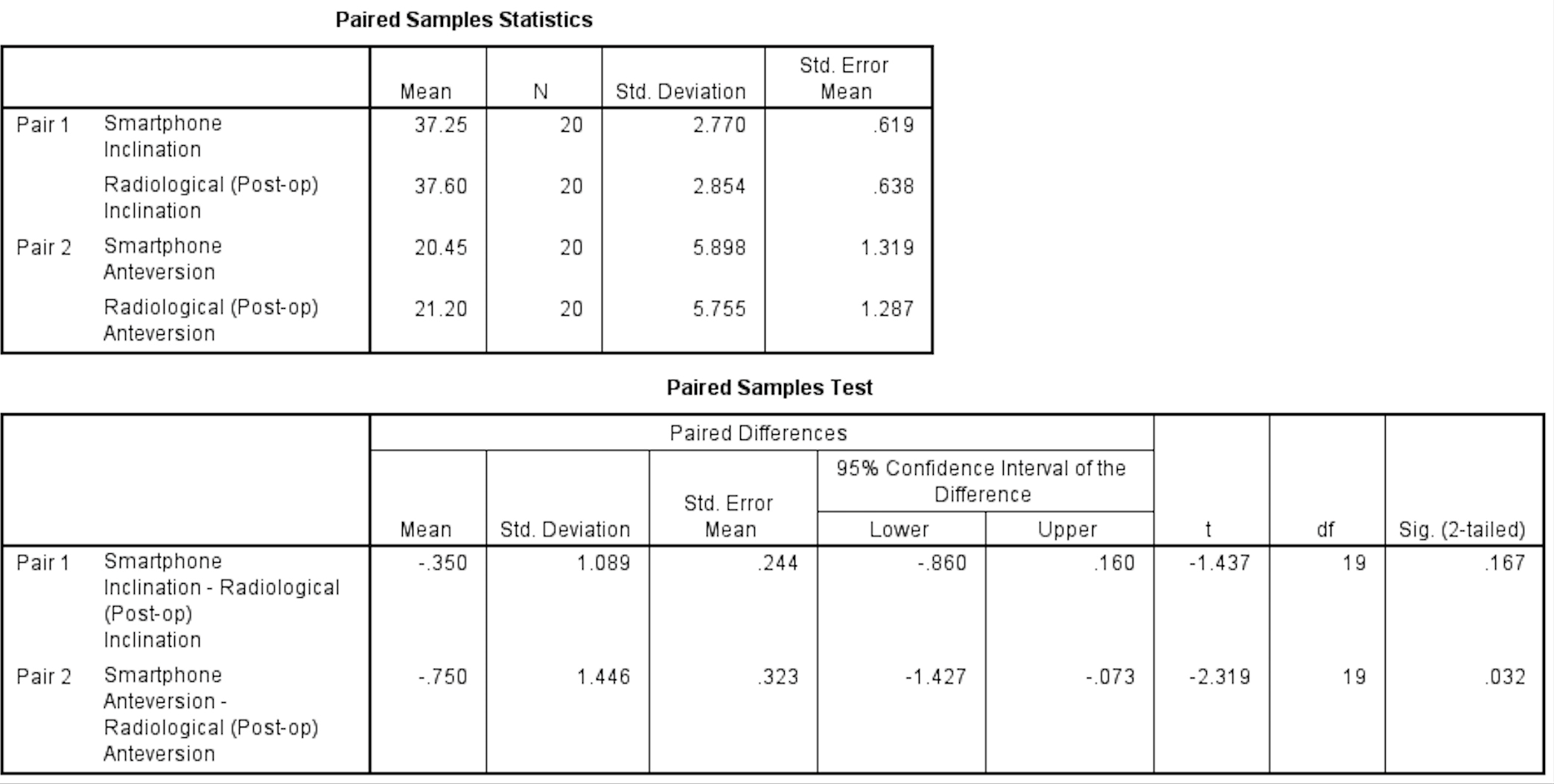
We used this technique in 20 consecutive cases and found the angles measured per operatively to correspond to the angles of inclination and anteversion measured on post operative scans within 3 degrees in each case. The mean Smartphone inclination angle was 37.25 (SD 2.77) whereas the mean Radiological inclination angle was 37.60 (SD 2.85). The mean Smartphone anteversion angle was 20.45 (SD 5.90) and the post op Radiological anteversion angle averaged 21.20 (SD 5.76). The mean difference in inclination between per operative Smartphone measurement and post operative radiological measurement was -0.350 (P=0.16) whereas the difference in anteversion angle was -0.750 (P=0.03).
The results are presented in the table below (Table 1, 2).
Table 1: Results showing the orientation of the cup as measured per operatively and post operative, radiological cup orientation.
|
Serial number |
Smartphone Inclination |
Smartphone Anteversion |
Radiological (Post-op) Inclination |
Radiological (Post-op) Anteversion |
Difference in inclination |
Difference in anteversion |
|
1 |
36 |
23 |
36 |
25 |
0 |
-2 |
|
2 |
35 |
27 |
35 |
27 |
0 |
0 |
|
3 |
42 |
30 |
41 |
28 |
1 |
2 |
|
4 |
35 |
22 |
35 |
20 |
0 |
2 |
|
5 |
36 |
25 |
35 |
25 |
1 |
0 |
|
6 |
39 |
20 |
39 |
23 |
0 |
-3 |
|
7 |
32 |
15 |
31 |
17 |
1 |
-2 |
|
8 |
35 |
15 |
36 |
15 |
-1 |
0 |
|
9 |
40 |
22 |
42 |
23 |
-2 |
-1 |
|
10 |
38 |
20 |
39 |
21 |
1 |
-1 |
|
11 |
41 |
15 |
40 |
18 |
-1 |
-3 |
|
12 |
36 |
11 |
37 |
10 |
-1 |
1 |
|
13 |
38 |
21 |
38 |
22 |
0 |
-1 |
|
14 |
40 |
15 |
42 |
15 |
-2 |
0 |
|
15 |
33 |
27 |
35 |
27 |
-2 |
0 |
|
16 |
35 |
23 |
36 |
25 |
-1 |
-2 |
|
17 |
41 |
30 |
40 |
31 |
1 |
-1 |
|
18 |
36 |
10 |
36 |
12 |
0 |
-2 |
|
19 |
39 |
15 |
39 |
15 |
0 |
0 |
|
20 |
38 |
23 |
40 |
25 |
-2 |
-2 |
Table 2: Paired sample T test was used to check for statistical significance. Since this study was done to validate our technique, we hypothesized that there would be no difference between the Smartphone and radiological angles (i.e., Null hypothesis). The P value for difference in inclination was 0.16, proving the null hypothesis, whereas the P value for difference in anteversion was 0.03. This could be owing to the fact that range of anteversion angle was wider (min 10 and max 30).
Discussion
Positioning of the acetabular cup is one of the most important factors influencing the outcome of Total hip replacement1,2,3. Various safe zones have been described in literature to achieve optimal results. These safe zones have varied from 20 to 55 degrees of inclination and 0 to 40 degrees of anteversion11. The most widely accepted safe zone has been described by Lewinnek et al.4.
Various factors can influence cup placement during surgery including intra-operative pelvic positioning, changes in the pelvic tilt that may take place during the procedure, and surgeon controlled positioning of the cup12. In this study, we have focused on the latter to improve cup placement.
Different techniques have been advocated to guide proper cup placement ranging from free hand technique to sophisticated computer or robotic navigation13. In our technique, we have utilized a humble smart phone and its camera function to guide the surgeon in assessing the positioning of the acetabular cup in terms of inclination and anteversion. This technique does not require usage of any additional app and has practically no learning curve.
We developed this technique keeping in mind our financial restrictions working in a public tertiary care hospital of a developing country. The purpose of our study was testing the accuracy and reliability of ‘No-touch smart phone technique’ in achieving the desire cup placement. We checked the positioning of the acetabular cup by taking intra operative pictures and compared it to the post op X-rays and CT scans to see if correlated with radiological measurement of cup inclination and anteversion. Results showed excellent correlation between the per operative angles and post op radiological assessment.
Similar concept has been used by various researchers using smart phone to guide the placement of acetabular cup with good results. All previous techniques quoted in literature use the accelerometer function of the smart phone and require manual handling of the device by the surgeon8,9,10. Pongkunakorn et al. conducted a study to compare cup orientation in two groups i.e., using smartphone applications and mechanical guides. They found that more cups from smartphone group corresponded to Lewinnick safe zone8. Peters et al. were able to position all acetabular cups in the target zone using smartphone technology10.
Such techniques described in literature require additional special equipment like a mounting brackets and sterilized pouches. Moreover, the surgeon has to place the smart phone in the desired position for measurement of relevant angles. We argue that such technique risks contamination of the surgical field and is time consuming. With advancements in smartphone cameras, angles measured using photographs taken by the smartphone have proven to be highly accurate as our study has demonstrated.
Our technique, is simple as anyone using a smart phone can take a satisfactory picture. The picture can easily be edited to make it parallel to the floor and hence horizontal (Figures 3,4 and 5). Then the angles can be measured using the markup function. It is also quick and does not take more than a couple of minutes. The sterile surgical field is not violated, and the surgical team can focus on the job at hand.
We found this technique to be more suitable for uncemented cups as there is ample time to change the position of the acetabular cup if the placement is outside the target zone. While using smartphone technique in guiding cemented acetabular components one has to be quick and efficient to minimize delay as cement hardens in a few minutes.
We acknowledge that this study could be simplifying the technical difficulties in acetabular cup placement. Studies have shown that many other factors like patient positioning, intra operative pelvic tilt, fixed spinal deformities, and anatomical variations also play a role. However, our purpose was to introduce an inexpensive, simple and reproducible technique which can be used to check cup positioning.
All techniques using smartphones assume that the position of the pelvis remains static during the procedure and that there is no spino-pelvic deformity. We did not use ‘No touch smartphone technique’ if pre op workup showed fixed deformities like scoliosis of kyphosis. For this purpose, all patients underwent thorough clinical examination and relevant radiological investigation pre operatively if and when required.
The main limitation of our study is the admittedly small sample size of 20 patients. However, once we found this simple technique to be surprisingly accurate and reliable, we planned to publish it so that other centers can use it and inform us about their experiences.
We advise that such low-cost techniques can be used to train young surgeons in proper component positioning where hi-tech computer navigation systems are not available.
Acknowledgement
The authors have no relevant disclosures to make and have not received any funding from any individual or company.
References
- Najarian BC, Kilgore JE, Markel DC. Evaluation of component positioning in primary total hip arthroplasty using an imageless navigation device compared with traditional methods. The Journal of arthroplasty. 2009; 24(1): 15-21.
- Moskal JT, Capps SG. Improving the accuracy of acetabular component orientation: avoiding malposition. JAAOS-Journal of the American Academy of Orthopaedic Surgeons. 2010; 18(5): 286-96.
- DiGioia AM, Jaramaz B, Blackwell M, et al. Image guided navigation system to measure intraoperatively acetabular implant alignment. Clinical Orthopaedics and Related Research®. 1998; 355: 8-22.
- Lewinnek GE, Lewis JL, Tarr RI, et al. Dislocations after total hip-replacement arthroplasties. J Bone Joint Surg Am. 1978; 60(2): 217-20.
- Hohmann E, Bryant A, Tetsworth K. A comparison between imageless navigated and manual freehand technique acetabular cup placement in total hip arthroplasty. The Journal of arthroplasty. 2011; 26(7): 1078-82.
- Gandhi R, Marchie A, Farrokhyar F, et al. Computer navigation in total hip replacement: a meta-analysis. International orthopaedics. 2009; 33(3): 593-7.
- Bosker BH, Verheyen CC, Horstmann WG, et al. Poor accuracy of freehand cup positioning during total hip arthroplasty. Archives of orthopaedic and trauma surgery. 2007; 127(5): 375-9.
- Pongkunakorn A, Chatmaitri S, Diewwattanawiwat K. Use of smartphone to improve acetabular component positioning in total hip athroplasty: A comparative clinical study. Journal of Orthopaedic Surgery. 2019; 27(1): 2309499019825578.
- Kurosaka K, Fukunishi S, Fukui T, et al. Assessment of accuracy and reliability in acetabular cup placement using an iPhone/iPad system. Orthopedics. 2016; 39(4): e621-6.
- Peters FM, Greeff R, Goldstein N, et al. Improving acetabular cup orientation in total hip arthroplasty by using smartphone technology. The Journal of arthroplasty. 2012; 27(7): 1324-30.
- Ishidou Y, Hirotsu M, Setoguchi T, et al. A Kirschner wire as a transverse-axis guide to improve acetabular cup positioning. Journal of Orthopaedic Surgery. 2016; 24(1): 22-6.
- Nishikubo Y, Fujioka M, Ueshima K, et al. Preoperative fluoroscopic imaging reduces variability of acetabular component positioning. The Journal of arthroplasty. 2011; 26(7): 1088-94.
- Xu K, Li YM, Zhang HF, et al. Computer navigation in total hip arthroplasty: a meta-analysis of randomized controlled trials. International Journal of Surgery. 2014; 12(5): 528-33.
- Khalifa AA, Bakr HM, Said E, et al. Technical Note on Using Intraoperative Smartphone Applications to Adjust Cup Inclination Angle during Total Hip Arthroplasty (THA). Archives of Bone and Joint Surgery. 2020; 8(6): 734. Available from: https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC7718568
- Ahmed AM, Khalifa AA. Orthopaedic Surgeons and Smartphones. International Journal of Recent Surgical and Medical Sciences. 2019; 05(01): 004-5.
- Khalifa AA, Abdelnasser MK, Ahmed AM, et al. Smartphone Application Helps Improve the Accuracy of Cup Placement by Young, Less-Experienced Surgeons during Primary Total Hip Arthroplasty. The Archives of Bone and Joint Surgery. 2022; 10(3): 278-85. Available from: https://abjs.mums.ac.ir/article_18648.html
- McArthur B, Cross M, Geatrakas C, et al. Measuring Acetabular Component Version After THA: CT or Plain Radiograph? Clinical Orthopaedics and Related Research. 2012; 470(10): 2810. Available from: https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC3441984/