
Low Rates of Reporting and Analyzing Race and Ethnicity in Hand Surgery Randomized Controlled Trials: A Systematic Review
Aneesh G. Patankar1*, Suleiman Y. Sudah2, Christopher R. Michel2, David S. Constantinescu3, Mariano E. Menendez4, Jeremy B. Ruskin5, Ajul Shah6
1Rutgers, Robert Wood Johnson Medical School, Piscataway, NJ, USA
2Department of Orthopedics, Monmouth Medical Center, Long Branch, NJ, USA
3Department of Orthopedic Surgery, University of Miami, Miami, FL, USA
4Midwest Orthopaedics at Rush, Rush University, Chicago, IL, USA
5Central Jersey Hand Surgery, Eatontown, NJ, USA
6The Center for Hand and Upper Extremity Surgery, Institute for Advanced Reconstruction, Shrewsbury, NJ, USA
Abstract
Purpose: Sociodemographic factors have been shown to influence musculoskeletal health. However, little is known regarding the frequency of reporting and analysis of certain sociodemographic variables (e.g., age, sex, height, weight, body mass index (BMI), race, and ethnicity) in randomized clinical trials (RCTs) pertaining to hand surgery. The purpose of this study was to assess the rate of reporting and analysis of these variables in RCTs published in the Journal of Hand Surgery (JHS).
Methods: A systematic review was conducted of RCTs published in JHS between 2015 and 2021. For each study, we determined whether the following sociodemographic variables were reported and/or analyzed: age, sex, height, weight, BMI, race, and ethnicity. Frequencies were reported by year and as a cumulative total. Studies were evaluated using the Cochrane risk-of-bias tool.
Results: A total of 45 RCTs met inclusion criteria, with about half (53.3%) originating from the United States. Age (97.8%) and sex (91.1%) were the most frequently reported sociodemographic variables, followed by race (17.8%), BMI (11.1%), and ethnicity (8.9%). Age (17.8%) was the most frequently analyzed variable, followed by sex (13.3%), and race (4.4%); the remaining variables were not analyzed in any study.
Conclusions: While age and sex are reported at a high rate, only about 1 in 4 RCTs published in JHS report either race or ethnicity. All sociodemographic variables were infrequently included as part of statistical analysis. The significance of these findings should be recognized and used to interpret and enhance the methodology of future RCTs.
Introduction
The influence of race and ethnicity on healthcare disparity is well-recognized within the medical community and has become a growing focus within the orthopedic literature1-7. The influence of race and ethnicity on postoperative outcomes following joint and spine surgery has been particularly elucidated. Adelani et al. retrospectively reviewed postoperative complications in 585,269 patients who underwent hip and knee arthroplasty. Within this study, Black patients experienced increased rates of surgical site infection (SSI), deep vein thrombosis (DVT), pulmonary embolism (PE), myocardial infarction, stroke, and death, even when controlling for medical comorbidities5. In a separate retrospective review of 4,803 patients, Sanford et al. found that Native American race was found to be an independent risk factor for SSI following cervical fusion and decompression laminectomy, whereas African American race was found to be an independent risk factor for SSI and PE after decompression laminectomy and DVT after lumbar fusion2. Alosh et al. screened over 100 million hospital discharge records from 1992 and 2005 and found 965,600 anterior cervical spine procedures. The authors similarly found that minorities had lower rates of surgery and that Black patients had significantly higher odds of dying while in the hospital6. Racial and ethnic differences in outcomes, decision-making, and other aspects in hand surgery itself further illustrate the health disparities within the field8-13.
Despite racial differences in health outcomes within the orthopedic literature, many randomized controlled trials (RCTs) fail to report race and ethnicity14,15. Several reasons for this observation have been postulated, such as the belief that reporting these factors is not clinically relevant and a lack of emphasis to report by medical journals15. However, according to the Consolidated Standards of Reporting Trials (CONSORT) guidelines for transparent reporting of clinical trials, all sociodemographic information should be provided in the initial description of a study population16. Similarly, the National Institutes of Health (NIH) guidelines require that minority patients be included in NIH-funded research and suggest that race and ethnicity be collected even in cases where previous research has demonstrated no effect of these variables on the outcomes of an intervention15.
It is important to identify racial and ethnic differences within orthopedic studies so that further analyses may elucidate the underlying causes of differential health outcomes. While some studies have assessed the reporting and analysis of sociodemographic variables across orthopedic subspecialty areas, none have focused on hand surgery specifically. The Journal of Hand Surgery (American Volume) (JHS) is a premier journal in this field with the largest number of RCTs on PubMed search relative to similar journals. For this reason, the purpose of our study was to assess the rate of reporting and analysis of sociodemographic variables (e.g., age, sex, height, weight, body mass index (BMI), race, and ethnicity) in RCTs published in JHS from 2015 to 2021. We hypothesize that age and sex will be reported and analyzed at the highest frequency compared to the other sociodemographic variables.
Methods
Search Strategy
The Preferred Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines were used to conduct this systematic review17 (Supplementary Table 1). This review was not prospectively registered. An advanced search on PubMed was conducted to identify all RCTs published in JHS from 2015 to 2021. Search terms included “randomized control trial” and “randomized controlled trial.” Search results were screened to confirm use of an RCT design.
Inclusion and Exclusion Criteria
All RCTs published in JHS between 2015 and 2021 on human subjects were included. We chose this span of years to reflect continuity with previous orthopedic studies on this topic, which included data from 2015 to their respective dates of publication14,15. Longitudinal analysis and previous follow-ups of clinical trials published prior to 2015 were included. Exclusion criteria were non-RCTs, basic science studies, meeting abstracts, responses to authors, letters to the editor, and withdrawn studies.
Data Collection
Eligible studies were assessed independently by two reviewers to determine whether the following sociodemographic variables were reported and/or analyzed: age, sex, height, weight, BMI, race, and ethnicity. Any discrepancy was resolved by consensus agreement with a senior author.
Data collection was based on the methodology reported by Griffin et al.14. A variable was considered reported if the mean or median with or without standard deviation/quartiles was provided for continuous variables (age, height, weight, BMI) or if a percentage of the study population was provided for categorical variables (sex, race, ethnicity). Comparing baseline demographics between treatment groups or between treatment and control groups was considered reporting but not analysis. A statement that all patients were of one race or ethnicity was considered adequate for reporting.
A variable was considered analyzed if statistical analysis was performed on the variable relative to the study’s outcomes of interest. The evaluation of outcomes based on sociodemographic subgroups was considered analysis. If a variable was found not to be analyzed throughout the included papers, this indicated that no figure or table was included with the variable as part of a sub-analysis, no mention of an analysis with respect to the variable was found throughout the Methods or other sections within the study, nor were any conclusions drawn regarding the sociodemographic variable’s impact on analyzed outcomes.
Race was defined using the following categories: White, African-American/Black, Asian/Pacific Islander, Native American, or other/unknown race. Ethnicity, which is defined as a subset of race, was defined as Hispanic or non-Hispanic18. Sex and gender were assessed as the same variable for the purpose of this study, as distinction between these terms is often interchangeable within the literature19. Each study’s country of origin was also recorded, with the institution of the senior author considered the country of origin when authors from multiple countries contributed to a study.
Risk-of-Bias Assessment
The revised Cochrane risk-of-bias tool for randomized trials (RoB 2.0) was used to assess each included study as “high risk,” “low risk,” or with “some concerns,” of bias. This tool evaluates the methodology of each study by scoring the following categories: randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, selection of the reported result, and overall bias20. Studies were assessed based on adherence to intention-to-treat analysis as this statistical method allows for optimal comparison between treatment groups and minimizes sources of bias21.
Results
Search Results
A total of 10,380 studies published in JHS were initially screened. 179 RCTs were identified, of which 45 met inclusion criteria and were included in the final review (Figure 1). Studies originating from 15 countries were included, the most common of which were the United States (53.3%), Denmark (6.7%), and Sweden (6.7%) (Figure 2). Most RCTs included in this review were published in 2017 (26.7%) and fewest were published in 2016 (4.4%) (Figure 3). Supplementary Table 2 compiles all included studies and illustrates data collected from each article.
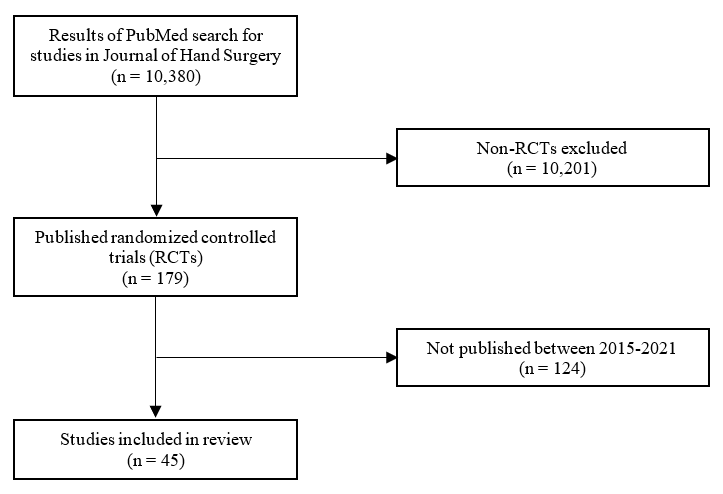
Figure 1: Flowchart of article inclusion
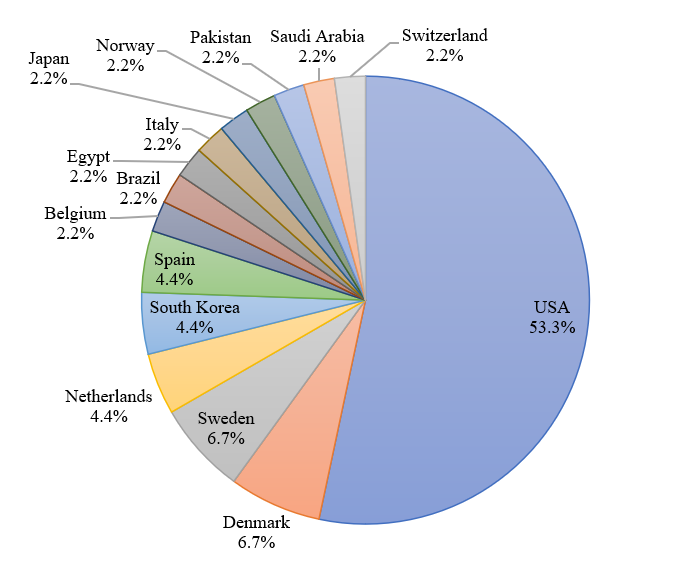
Figure 2: Country of origin for included RCTs
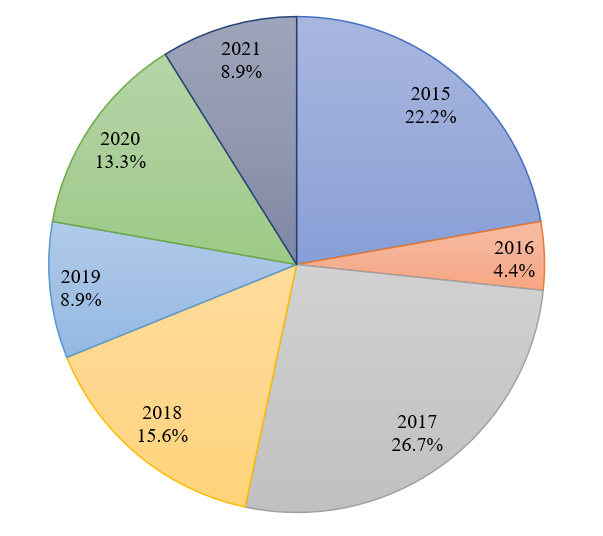
Figure 3: Year of publication for included RCTs
Reporting of Sociodemographic Variables
Of the 45 included studies, 44 reported age (97.8%), 41 reported sex (91.1%), eight reported race (17.8%), five reported BMI (11.1%), four reported ethnicity (8.9%), one reported height (2.2%), and one reported weight (2.2%) (Figure 4).
Sociodemographic reporting trended upward with time (Figure 5). Age and sex were reported at a high rate for each year of the study period, with both variables being reported in all studies since 2019. The reporting of race was variable year to year but trended upward with time, from 11.1% in 2015 to 25% in 2021. Ethnicity was only reported in 2017 (16.7%), 2020 (16.7%), and most frequently in 2021 (25%), and no specific trends could be observed. The proportions of sociodemographic reporting by year can be found in Supplementary Table 3.
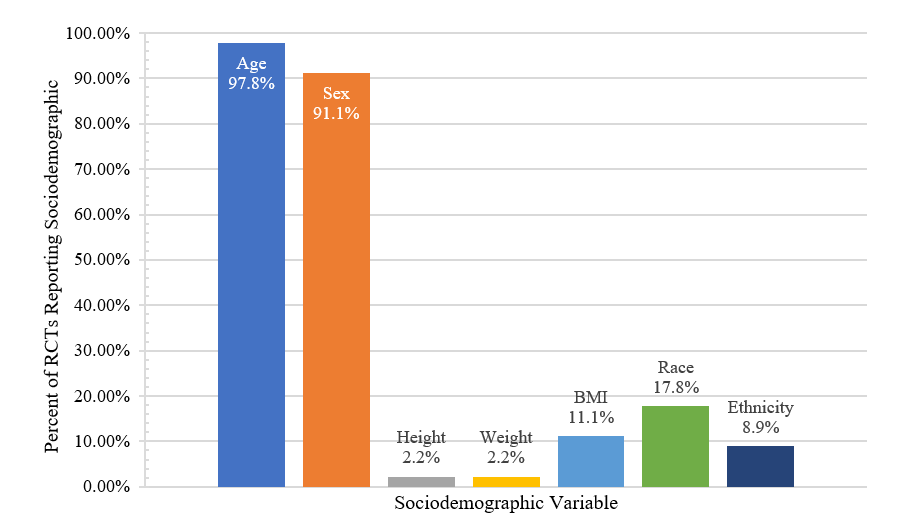
Figure 4: Proportion of studies reporting sociodemographic variables
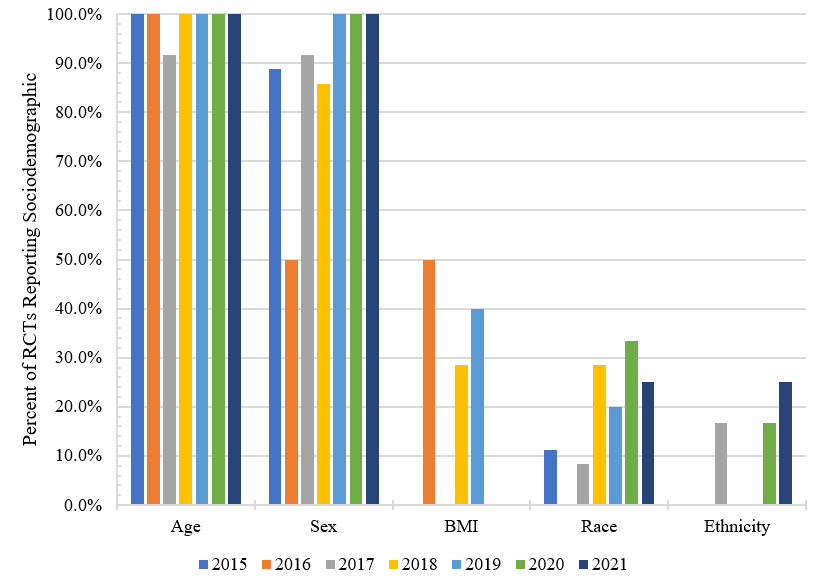
Figure 5: Proportion of studies reporting sociodemographic variables separated by year of publication
Analysis of Sociodemographic Variables
The most analyzed sociodemographic variable was age (n=8; 17.8%), followed by sex (n=6; 13.3%) and race (n=2; 4.4%) (Figure 6). No studies analyzed weight, height, BMI, or ethnicity. No specific trends could be observed for the analysis of the variables when separated by year of publication (Figure 7). The proportions of sociodemographic analysis by year can be found in Supplementary Table 4. Figure data is also summarized in Supplementary Table 5 to allow for accurate, additional interpretation of the provided figures.
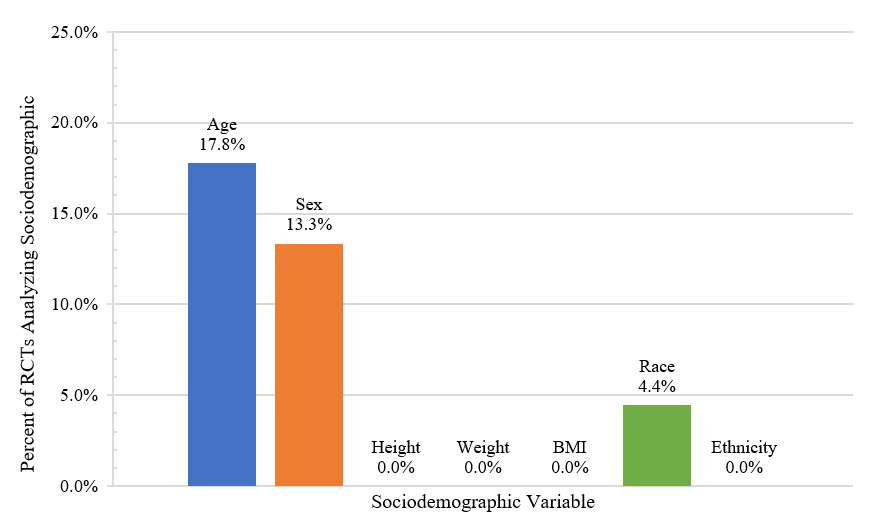
Figure 6: Proportion of studies analyzing sociodemographic variables
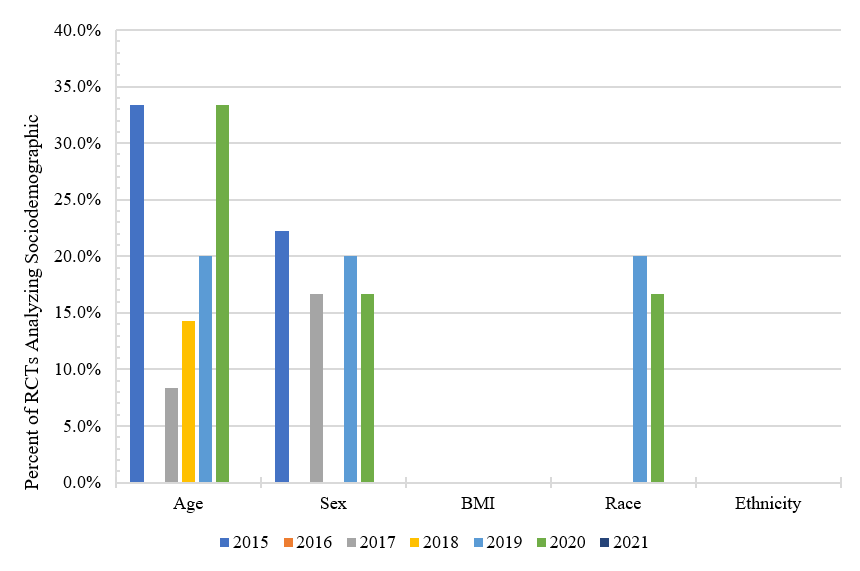
Figure 7: Proportion of studies analyzing sociodemographic variables separated by year of publication
Risk of Bias
“Selection of the reported result” had the least bias, with 95.6% of studies in this category classified as low risk (Figure 8). Most studies (>84%) had low levels of bias with respect to “deviations from intended outcomes,” “missing outcome data,” and their “randomization process.” “Measurement of the outcome” revealed some concerns for bias in 31.1% of studies.
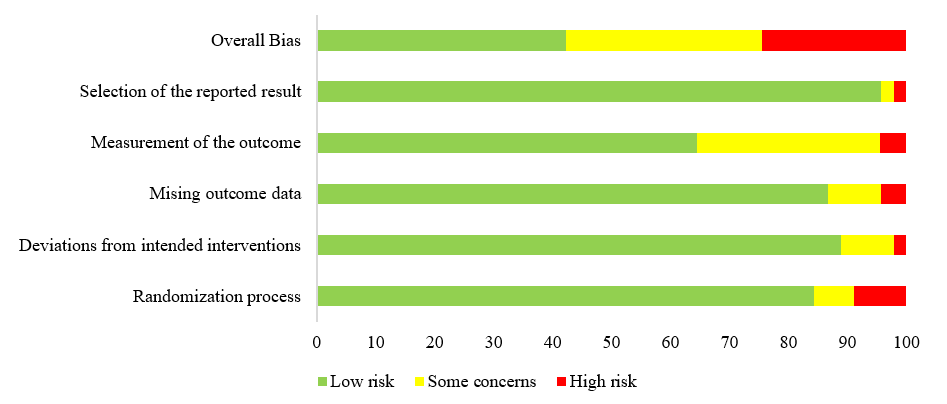
Figure 8: Bias assessment of included studies using the Cochrane risk-of-bias tool
Discussion
The primary purpose of this study was to evaluate the frequency of reporting and analyzing of several sociodemographic variables in hand surgery RCTs published in JHS between 2015 and 2021. Age and sex were the most reported demographics and were presented in nearly every study. Interestingly, race was reported in about one of six studies, while ethnicity was reported half as often. Height and weight were most infrequently reported but included through BMI in more than 10% of studies. Despite high rates of reporting, age was included within the statistical analysis of only 17.8% of studies, followed by sex in 13.3%, and race in 4.4%. There was no analysis of ethnicity, height, weight, or BMI throughout the seven-year period.
A recent systematic review investigated the rates at which randomized controlled trials published in 10 orthopedic journals between 2015 and 2019 reported and analyzed these same sociodemographic variables15. Of 482 total articles, only 7.3% reported race and 3.1% reported ethnicity. Analysis by race (1.2%) and ethnicity (0.2%) were much less frequent. Within this same study, articles were further subdivided into subspecialty categories. Of the 12 articles pertaining to hand surgery, 8.3% reported race and no studies reported ethnicity; each of these studies failed to perform analysis of these demographics. Interestingly, we found that RCTs published in JHS over a similar period reported race (17.8%) and ethnicity (8.9%) at much higher frequencies. These findings imply that rates of sociodemographic reporting may vary amongst RCTs of different orthopedic journals even if they pertain to the same orthopedic domain. Further study of specialty-specific journals should be performed to increase the power of these results and more accurately identify the rate of reporting and analysis of sociodemographic variables14.
In reviewing the racial and ethnic demographics of included publications within our study, we found there to be great diversity but inconsistent reporting of included patients22-29. For example, of the eight RCTs that reported race, half provided data on the number of White versus non-White patients22,24-26 only, while half provided data on a larger variety of subgroups including White, Black, Asian, Native American, and Pacific Islander patients23,27-29. Only three studies reported ethnicity by including the percentage of Hispanic patients within their study populations23,28,29, while one study commented on the ‘ethnic homogeneity’ of its study population30. Regarding analysis of race and ethnicity, only two of the 45 studies (4.4%) within this review analyzed outcomes based on race, and none analyzed outcomes based on ethnicity.
As discussed previously, race has been shown to impact joint and spine surgery in the field of orthopaedic surgery2,5,6. However, other studies have explored the effect of race and ethnicity on the outcomes, decision-making, and other aspects of hand surgery. In a retrospective review of 92,921 patients with carpal tunnel syndrome, Brodeur et al. found that Black and Asian patients were less likely to undergo surgery compared to White patients. Similarly, the authors showed that patients of Hispanic ethnicity had decreased odds of surgery compared to patients of non-Hispanic ethnicity31. Mahmoudi et al. retrospectively reviewed 13,129 patients with traumatic digit amputation and found that Black patients were less likely than White patients to undergo replantation procedures32. In a separate analysis of over 31,000 trigger finger patients by Brodeur et al., Asian, African American, and other minority patients were less likely to undergo surgery relative to White patients9. Squitieri et al. similarly showed that Black and Hispanic children underwent attempted reimplantation of an amputated finger at significantly lower rates than their White counterparts, even after controlling for potential confounding factors11. Following a brachial plexus injury, Bucknor et al. found that Black patients are more likely to be treated in the emergency department as opposed to an elective, outpatient setting and are also less likely to receive supported discharge compared to White patients12. Walsh et al. found that Black and Hispanic patients show worse functional outcomes and report higher levels of pain following a distal radius fracture relative to White patients10 while a review by Khetpal et al. revealed many outcomes affected by various sociodemographic variables, including race13.
These studies illustrate the disparities in treatment rate and outcomes, among other factors, that are associated with the race and ethnicity of the patient. By highlighting these findings, we hope to emphasize the presence of these health inequities and stress the importance of analyzing—or at least reporting—these sociodemographic variables for future RCTs. Because race and ethnicity have been shown to affect patient decision-making and outcomes and may affect access to healthcare or the biases that patients experience, study outcomes should take into account these potential moderating factors. Not only can this reveal other yet-undiscovered health inequities, but it can also lead to treatments optimized for the patient’s race and prevent complications disproportionately affecting particular minorities.
While race was infrequently reported and analyzed even less often, age was the most frequently analyzed sociodemographic variable in our review. Many of the included studies show that age, like race, can impact outcomes, decision-making, and other aspects in hand surgery. In a mixed-methods study by Zhuang et al., participants were asked to choose between receiving carpal tunnel release (expensive) or orthosis wear (inexpensive) for hypothetical carpal tunnel symptoms after either receiving or not receiving cost information regarding the procedure. After stratifying the participants based on age, the younger subgroup was more inclined to choose surgery despite exposure to cost information when compared to the older subgroup23. Valdes et al. investigated whether there was a difference in postoperative outcomes following volar plate fixation for distal radius fractures in patients randomized to home (unsupervised) vs. therapist-supervised hand therapy. Overall, there were no statistically significant differences in self-evaluation scores, extremity motion, pain, or grip strength. However, older subjects had poorer grip and self-evaluation scores at 12 weeks and reported less pain when compared to younger subjects33. Finally, Chung et al. studied the predictors of outcomes 12 months following distal radius fractures. The authors found that increasing age was associated with lower Michigan Hand Questionnaire scores, implying that older patients with distal radius fractures may expect poorer outcomes when compared to those of younger age27.
These findings show that outcomes of hand surgery RCTs can be heavily influenced by age. Differences based on other sociodemographic variables may be elucidated with increased reporting and analysis. Researchers should focus on the identification of health disparity so that clinicians can more effectively counsel patients before and after treatment.
The conclusions of our study may be limited by the small sample size of RCTs that met the inclusion criteria. Though all RCTs between 2015 and 2021 published in JHS were included, additional years of data collection or inclusion of other study types – such as highly powered cohort studies15 – may help to reveal racial and ethnic differences. Similarly, only papers published in JHS were included in this study; future studies should explore these sociodemographic trends in other hand surgery journals. As JHS is based in the United States, there may be some bias in the rate of publishing of studies submitted from the journal’s home country, potentially skewing the geographical distribution of recent hand literature. Studies published in non-US-based hand surgery journals can be evaluated in future studies to explore this possible bias. In addition, there are a variety of socioeconomic factors associated with patient race and ethnicity that may influence study outcomes and never be adequately considered34,35. As such, the effect of biological versus social factors on health outcomes remains difficult. Finally, included studies may have forgone the evaluation of race or ethnicity if these differences were known to have negligible effect on the intervention. Future reviews can select studies associated with topics known to exhibit notable health differences amongst these variables.
Conclusions
The present review of RCTs published in JHS between 2015 and 2021 found that the sociodemographic variables of age and sex were reported at high rates. Conversely, race was less commonly reported, and ethnicity was rarely reported. Each variable was infrequently included as part of statistical analysis. Because outcomes of hand surgery RCTs can be heavily influenced by race and age and may be further moderated by other sociodemographic variables, both reporting and analysis of these variables is crucial to ensure accurate and comprehensive study conclusions. The significance of these findings should be recognized and used to interpret and enhance the methodology of future RCTs.
Conflict of Interest
The Authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
- Braveman P, Egerter S, Williams DR. The social determinants of health: coming of age. Annu Rev Public Health. 2011; 32: 381-98. doi:10.1146/annurev-publhealth-031210-101218
- Sanford Z, Taylor H, Fiorentino A, et al. Racial Disparities in Surgical Outcomes After Spine Surgery: An ACS-NSQIP Analysis. Global Spine J. 2019; 9(6): 583-590. doi:10.1177/2192568218811633
- Nelson CL. Disparities in Orthopaedic Surgical Intervention. JAAOS - Journal of the American Academy of Orthopaedic Surgeons. 2007. doi:10.5435/00124635-200700001-00005
- Pandya NK, Wustrack R, Metz L, et al. Current Concepts in Orthopaedic Care Disparities. JAAOS - Journal of the American Academy of Orthopaedic Surgeons. 2018; 26(23): 823-832. doi:10.5435/JAAOS-D-17-00410
- Adelani MA, Archer KR, Song Y, et al. Immediate Complications Following Hip and Knee Arthroplasty: Does Race Matter? The Journal of Arthroplasty. 2013; 28(5): 732-735. doi:10.1016/j.arth.2012.09.015
- Alosh H, Riley LH 3rd, Skolasky RL. Insurance Status, Geography, Race, and Ethnicity as Predictors of Anterior Cervical Spine Surgery Rates and In-Hospital Mortality: An Examination of United States Trends From 1992 to 2005. Spine. 2009; 34(18): 1956-62. doi:10.1097/BRS.0b013e3181ab930e
- Schoenfeld AJ, Tipirneni R, Nelson JH, et al. The Influence of Race and Ethnicity on Complications and Mortality After Orthopedic Surgery: A Systematic Review of the Literature. Medical Care. 2014; 52(9): 842-51. doi:10.1097/MLR.0000000000000177
- Brodeur PG, Patel DD, Raducha JE, et al. Social Disparities in the Management of Trigger Finger: An Analysis of 31, 411 Cases. AAHS Annual Meeting 2022.
- Brodeur PG, Patel DD, Licht AH, et al. Demographic Disparities amongst Patients Receiving Carpal Tunnel Release: A Retrospective Review of 92,921 Patients. Plastic and Reconstructive Surgery – Global Open. 2021; 9(11): e3959. doi:10.1097/gox.0000000000003959
- Walsh M, Davidovitch RI, Egol KA. Ethnic Disparities in Recovery Following Distal Radial Fracture. JBJS. 2010; 92(5): 1082-1087. doi:10.2106/jbjs.H.01329
- Squitieri L, Reichert H, Kim HM, et al. Patterns of surgical care and health disparities of treating pediatric finger amputation injuries in the United States. J Am Coll Surg. 2011; 213(4): 475-85. doi:10.1016/j.jamcollsurg.2011.07.017
- Bucknor A, Huang A, Wu W, et al. Socioeconomic Disparities in Brachial Plexus Surgery: A National Database Analysis. Plastic and Reconstructive Surgery – Global Open. 2019; 7(2): e2118. doi:10.1097/gox.0000000000002118
- Khetpal S, Lopez J, Redett RJ, et al. Health Equity and Healthcare Disparities in Plastic Surgery: What We Can Do. Journal of Plastic, Reconstructive & Aesthetic Surgery. 2021; 74(12): 3251-3259. doi:10.1016/j.bjps.2021.05.026
- Griffin SA, Magnuson JA, Sutton RM, et al. Reporting and Analyzing Demographics in the Journal of Arthroplasty: Are We Making Progress? J Arthroplasty. 2021; 36(12): 3825-3830. doi:10.1016/j.arth.2021.09.017
- Paul RW, Lee D, Brutico J, et al. Reporting and Analyzing Race and Ethnicity in Orthopaedic Clinical Trials: A Systematic Review. J Am Acad Orthop Surg Glob Res Rev. 2021; 5(5): e21.00027. doi:10.5435/JAAOSGlobal-D-21-00027
- Group TC. Baseline Data. Accessed February 6, 2022. http://www.consort-statement.org/checklists/view/32--consort-2010/510-baseline-data
- Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021; 372: n71. doi:10.1136/bmj.n71
- Winker MA. Measuring Race and Ethnicity: Why and How? JAMA. 2004; 292(13): 1612-1614. doi:10.1001/jama.292.13.1612
- Clayton JA, Tannenbaum C. Reporting Sex, Gender, or Both in Clinical Research? JAMA. 2016; 316(18): 1863-1864. doi:10.1001/jama.2016.16405
- Sterne JAC, SavoviÄ J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. Bmj. 2019; 366: l4898. doi:10.1136/bmj.l4898
- Ranganathan P, Pramesh CS, Aggarwal R. Common pitfalls in statistical analysis: Intention-to-treat versus per-protocol analysis. Perspect Clin Res. 2016; 7(3): 144-146. doi:10.4103/2229-3485.184823
- Tyser AR, Beckmann J, Weng C, et al. A randomized trial of the disabilities of the arm, shoulder, and hand administration: tablet computer versus paper and pencil. J Hand Surg Am. 2015; 40(3): 554-9. doi:10.1016/j.jhsa.2014.10.046
- Zhuang T, Kortlever JTP, Shapiro LM, et al. The Influence of Cost Information on Treatment Choice: A Mixed-Methods Study. J Hand Surg Am. 2020; 45(10): 899-908. doi:10.1016/j.jhsa.2020.05.019
- Wilkens SC, Ring D, Teunis T, et al. Decision Aid for Trapeziometacarpal Arthritis: A Randomized Controlled Trial. J Hand Surg Am. 2019; 44(3): 247. doi:10.1016/j.jhsa.2018.06.004
- Keulen MHF, Teunis T, Vagner GA, et al. The Effect of the Content of Patient-Reported Outcome Measures on Patient Perceived Empathy and Satisfaction: A Randomized Controlled Trial. J Hand Surg Am. 2018; 43(12): 1141. doi:10.1016/j.jhsa.2018.04.020
- Kleiss IIM, Kortlever JTP, Ring D, et al. A Randomized Controlled Trial of Decision Aids for Upper-Extremity Conditions. J Hand Surg Am. 2021; 46(4): 338. doi:10.1016/j.jhsa.2020.09.003
- Chung KC, Kim HM, Malay S, et al. Predicting Outcomes After Distal Radius Fracture: A 24-Center International Clinical Trial of Older Adults. J Hand Surg Am. 2019; 44(9): 762-771. doi:10.1016/j.jhsa.2019.05.016
- Curtin CM, Kenney D, Suarez P, et al. A Double-Blind Placebo Randomized Controlled Trial of Minocycline to Reduce Pain After Carpal Tunnel and Trigger Finger Release. J Hand Surg Am. 2017; 42(3): 166-174. doi:10.1016/j.jhsa.2016.12.011
- Roe AK, Eppler SL, Shapiro LM, et al. Engaging Patients to Ask More Questions: What's the Best Way? A Pragmatic Randomized Controlled Trial. J Hand Surg Am. 2021; 46(9): 818. doi:10.1016/j.jhsa.2021.02.001
- Skov ST, Bisgaard T, Søndergaard P, et al. Injectable Collagenase Versus Percutaneous Needle Fasciotomy for Dupuytren Contracture in Proximal Interphalangeal Joints: A Randomized Controlled Trial. J Hand Surg Am. 2017; 42(5): 321-328.e3. doi:10.1016/j.jhsa.2017.03.003
- Brodeur PG, Patel DD, Licht AH, et al. Demographic Disparities amongst Patients Receiving Carpal Tunnel Release: A Retrospective Review of 92,921 Patients. Plast Reconstr Surg Glob Open. 2021; 9(11): e3959. doi:10.1097/gox.0000000000003959
- Mahmoudi E, Swiatek PR, Chung KC, et al. Racial Variation in Treatment of Traumatic Finger/Thumb Amputation: A National Comparative Study of Replantation and Revision Amputation. Plast Reconstr Surg. 2016; 137(3): 576e-585e. doi:10.1097/01.prs.0000479969.14557.9d
- Valdes K, Naughton N, Burke CJ. Therapist-supervised hand therapy versus home therapy with therapist instruction following distal radius fracture. J Hand Surg Am. 2015; 40(6): 1110-6. doi:10.1016/j.jhsa.2015.01.036
- Caulfield T, Fullerton SM, Ali-Khan SE, et al. Race and ancestry in biomedical research: exploring the challenges. Genome Med. 2009; 1(1): 8. doi:10.1186/gm8
- Kaufman JS, Cooper RS. Race in epidemiology: new tools, old problems. Ann Epidemiol. 2008; 18(2): 119-23. doi:10.1016/j.annepidem.2007.09.002
- Alter TH, Ilyas AM. A Prospective Randomized Study Analyzing Preoperative Opioid Counseling in Pain Management After Carpal Tunnel Release Surgery. J Hand Surg Am. 2017; 42(10): 810-815. doi:10.1016/j.jhsa.2017.07.003
- Alter TH, Liss FE, Ilyas AM. A Prospective Randomized Study Comparing Bupivacaine Hydrochloride Versus Bupivacaine Liposome for Pain Management After Distal Radius Fracture Repair Surgery. J Hand Surg Am. 2017; 42(12): 1003-1008. doi:10.1016/j.jhsa.2017.08.022
- Badalamente MA, Hurst LC, Benhaim P, et al. Efficacy and safety of collagenase clostridium histolyticum in the treatment of proximal interphalangeal joints in dupuytren contracture: combined analysis of 4 phase 3 clinical trials. J Hand Surg Am. 2015; 40(5): 975-83. doi:10.1016/j.jhsa.2015.02.018
- Bashir MM, Qayyum R, Saleem MH, et al. Effect of Time Interval Between Tumescent Local Anesthesia Infiltration and Start of Surgery on Operative Field Visibility in Hand Surgery Without Tourniquet. J Hand Surg Am. 2015; 40(8): 1606-9. doi:10.1016/j.jhsa.2015.03.034
- Boriani F, Granchi D, Roatti G, et al. Alpha-lipoic Acid After Median Nerve Decompression at the Carpal Tunnel: A Randomized Controlled Trial. J Hand Surg Am. 2017; 42(4): 236-242. doi:10.1016/j.jhsa.2017.01.011
- Cantero-Téllez R, Cuesta-Vargas AI, Cuadros-Romero M. Treatment of proximal interphalangeal joint flexion contracture: combined static and dynamic orthotic intervention compared with other therapy intervention: a randomized controlled trial. J Hand Surg Am. 2015; 40(5): 951-5. doi:10.1016/j.jhsa.2015.01.005
- Dailey SK, Miller AR, Kakazu R, et al. The Effectiveness of Mini-C-Arm Fluoroscopy for the Closed Reduction of Distal Radius Fractures in Adults: A Randomized Controlled Trial. J Hand Surg Am. 2018; 43(10): 927-931. doi:10.1016/j.jhsa.2018.02.015
- Dale EL, Kluemper CT, Cowart SJ, et al. Bupivacaine Extended-Release Liposomal Injection Versus Bupivacaine HCl for Early Postoperative Pain Control Following Wrist Operations: A Prospective, Randomized Control Trial. J Hand Surg Am. 2020; 45(6): 550. doi:10.1016/j.jhsa.2019.10.009
- de Moraes VY, Queiroz J, Jr., Raduan-Neto J, et al. Nonsurgical Treatment for Symptomatic Carpal Tunnel Syndrome: A Randomized Clinical Trial Comparing Local Corticosteroid Injection Versus Night Orthosis. J Hand Surg Am. 2021; 46(4): 295-300. doi:10.1016/j.jhsa.2020.11.014
- Earp BE, Stanbury SJ, Mora AN, et al. Needle-Free Jet Lidocaine Administration for Preinjection Anesthesia in Trigger Finger Injection: A Randomized Controlled Trial. J Hand Surg Am. 2017; 42(8): 618-622. doi:10.1016/j.jhsa.2017.05.001
- El-Saeed M, Sallam A, Radwan M, et al. Kirschner Wires Versus Titanium Plates and Screws in Management of Unstable Phalangeal Fractures: A Randomized, Controlled Clinical Trial. J Hand Surg Am. 2019; 44(12): 1091. doi:10.1016/j.jhsa.2019.01.015
- Franko OI, Stern PJ. Use and Effectiveness of Ethyl Chloride for Hand Injections. J Hand Surg Am. 2017; 42(3): 175-181. doi:10.1016/j.jhsa.2016.12.013
- Hansen RL, Søndergaard M, Lange J. Open Surgery Versus Ultrasound-Guided Corticosteroid Injection for Trigger Finger: A Randomized Controlled Trial With 1-Year Follow-up. J Hand Surg Am. 2017; 42(5): 359-366. doi:10.1016/j.jhsa.2017.02.011
- Hegazy G, Massoud AH, Seddik M, et al. Structural Versus Nonstructural Bone Grafting for the Treatment of Unstable Scaphoid Waist Nonunion Without Avascular Necrosis: A Randomized Clinical Trial. J Hand Surg Am. 2021; 46(6): 462-470. doi:10.1016/j.jhsa.2021.01.027
- Hutchison RL, O'Rear J, Olson-Burgess C, et al. Offering the Influenza Vaccine in a Pediatric Hand Surgery Clinic Increases Vaccination Rates. J Hand Surg Am. 2018; 43(8): 776. doi:10.1016/j.jhsa.2018.01.017
- Ilyas AM, Miller AJ, Graham JG, et al. Pain Management After Carpal Tunnel Release Surgery: A Prospective Randomized Double-Blinded Trial Comparing Acetaminophen, Ibuprofen, and Oxycodone. J Hand Surg Am. 2018; 43(10): 913-919. doi:10.1016/j.jhsa.2018.08.011
- Keulen MHF, Teunis T, Vagner GA, et al. The Effect of the Content of Patient-Reported Outcome Measures on Patient Perceived Empathy and Satisfaction: A Randomized Controlled Trial. J Hand Surg Am. 2018; 43(12): 1141. doi:10.1016/j.jhsa.2018.04.020
- Kleiss IIM, Kortlever JTP, Ring D, et al. A Randomized Controlled Trial of Decision Aids for Upper-Extremity Conditions. J Hand Surg Am. 2021; 46(4): 338. doi:10.1016/j.jhsa.2020.09.003
- Landgren M, Abramo A, Geijer M, et al. Fragment-Specific Fixation Versus Volar Locking Plates in Primarily Nonreducible or Secondarily Redisplaced Distal Radius Fractures: A Randomized Controlled Study. J Hand Surg Am. 2017; 42(3): 156-165. doi:10.1016/j.jhsa.2016.12.001
- Logli AL, Bear BJ, Schwartz EG, et al. A Prospective, Randomized Trial of Splinting After Minicarpal Tunnel Release. J Hand Surg Am. 2018; 43(8): 775. doi:10.1016/j.jhsa.2018.01.016
- Marks M, Hensler S, Wehrli M, et al. Trapeziectomy With Suspension-Interposition Arthroplasty for Thumb Carpometacarpal Osteoarthritis: A Randomized Controlled Trial Comparing the Use of Allograft Versus Flexor Carpi Radialis Tendon. J Hand Surg Am. 2017; 42(12): 978-986. doi:10.1016/j.jhsa.2017.07.023
- Martínez-Catalán N, Pajares S, Llanos L, et al. A Prospective Randomized Trial Comparing the Functional Results of Buddy Taping Versus Closed Reduction and Cast Immobilization in Patients With Fifth Metacarpal Neck Fractures. J Hand Surg Am. 2020; 45(12): 1134-1140. doi:10.1016/j.jhsa.2020.05.013
- Nishiwaki M, Terasaka Y, Kiyota Y, et al. A Prospective Randomized Comparison of Variable-Angle and Fixed-Angle Volar Locking Plating for Intra-Articular Distal Radius Fractures. J Hand Surg Am. 2021; 46(7): 584-593. doi:10.1016/j.jhsa.2021.03.014
- Plate JF, Gaffney DL, Emory CL, et al. Randomized comparison of volar locking plates and intramedullary nails for unstable distal radius fractures. J Hand Surg Am. 2015; 40(6): 1095-101. doi:10.1016/j.jhsa.2015.02.014
- Roe AK, Eppler SL, Shapiro LM, et al. Engaging Patients to Ask More Questions: What's the Best Way? A Pragmatic Randomized Controlled Trial. J Hand Surg Am. 2021; 46(9): 818. doi:10.1016/j.jhsa.2021.02.001
- Roh YH, Lee BK, Baek JR, et al. A randomized comparison of volar plate and external fixation for intra-articular distal radius fractures. J Hand Surg Am. 2015; 40(1): 34-41. doi:10.1016/j.jhsa.2014.09.025
- Roh YH, Hwangbo K, Gong HS, et al. Comparison of Ultrasound-Guided Versus Landmark-Based Corticosteroid Injection for Carpal Tunnel Syndrome: A Prospective Randomized Trial. J Hand Surg Am. 2019; 44(4): 304-310. doi:10.1016/j.jhsa.2019.02.007
- Saving J, Enocson A, Ponzer S, et al. External Fixation Versus Volar Locking Plate for Unstable Dorsally Displaced Distal Radius Fractures-A 3-Year Follow-Up of a Randomized Controlled Study. J Hand Surg Am. 2019; 44(1): 18-26. doi:10.1016/j.jhsa.2018.09.015
- Schwartzenberger J, Presson A, Lyle A, et al. Remote Collection of Patient-Reported Outcomes Following Outpatient Hand Surgery: A Randomized Trial of Telephone, Mail, and E-Mail. J Hand Surg Am. 2017; 42(9): 693-699. doi:10.1016/j.jhsa.2017.05.002
- Selles CA, Beerekamp MSH, Leenhouts PA, et al. The Value of Intraoperative 3-Dimensional Fluoroscopy in the Treatment of Distal Radius Fractures: A Randomized Clinical Trial. J Hand Surg Am. 2020; 45(3): 189-195. doi:10.1016/j.jhsa.2019.11.006
- Soberón JR Jr, Crookshank JW 3rd, Nossaman BD, et al. Distal Peripheral Nerve Blocks in the Forearm as an Alternative to Proximal Brachial Plexus Blockade in Patients Undergoing Hand Surgery: A Prospective and Randomized Pilot Study. J Hand Surg Am. 2016; 41(10): 969-977. doi:10.1016/j.jhsa.2016.07.092
- Strömberg J, Ibsen-Sörensen A, Fridén J. Comparison of Treatment Outcome After Collagenase and Needle Fasciotomy for Dupuytren Contracture: A Randomized, Single-Blinded, Clinical Trial With a 1-Year Follow-Up. J Hand Surg Am. 2016; 41(9): 873-80. doi:10.1016/j.jhsa.2016.06.014
- Spekreijse KR, Vermeulen GM, Kedilioglu MA, et al. The Effect of a Bone Tunnel During Ligament Reconstruction for Trapeziometacarpal Osteoarthritis: A 5-Year Follow-up. J Hand Surg Am. 2015; 40(11): 2214-22. doi:10.1016/j.jhsa.2015.07.011
- Tsolias A, Detrembleur C, Druez V, et al. Effect of Radial Nerve Release on Lateral Epicondylitis Outcomes: A Prospective, Randomized, Double-Blinded Trial. J Hand Surg Am. 2019; 44(3): 216-221. doi:10.1016/j.jhsa.2018.06.009
- Valdes K, Naughton N, Burke CJ. Therapist-supervised hand therapy versus home therapy with therapist instruction following distal radius fracture. J Hand Surg Am. 2015; 40(6): 1110-6.e1. doi:10.1016/j.jhsa.2015.01.036
- Wasterlain AS, Melamed E, Bello R, et al. The Effect of Price on Surgeons' Choice of Implants: A Randomized Controlled Survey. J Hand Surg Am. 2017; 42(8): 593-601. doi:10.1016/j.jhsa.2017.05.005
- Weinheimer K, Michelotti B, Silver J, et al. A Prospective, Randomized, Double-Blinded Controlled Trial Comparing Ibuprofen and Acetaminophen Versus Hydrocodone and Acetaminophen for Soft Tissue Hand Procedures. J Hand Surg Am. 2019; 44(5): 387-393. doi:10.1016/j.jhsa.2018.10.014
- Wilkens SC, Ring D, Teunis T, et al. Decision Aid for Trapeziometacarpal Arthritis: A Randomized Controlled Trial. J Hand Surg Am. 2019; 44(3): 247.e1-247. doi:10.1016/j.jhsa.2018.06.004
- Williksen JH, Husby T, Hellund JC, et al. External Fixation and Adjuvant Pins Versus Volar Locking Plate Fixation in Unstable Distal Radius Fractures: A Randomized, Controlled Study With a 5-Year Follow-Up. J Hand Surg Am. 2015; 40(7): 1333-40. doi:10.1016/j.jhsa.2015.03.008
- Zhuang T, Kortlever JTP, Shapiro LM, et al. The Influence of Cost Information on Treatment Choice: A Mixed-Methods Study. J Hand Surg Am. 2020; 45(10): 899-908. doi:10.1016/j.jhsa.2020.05.019
Supplementary Table 1: PRISMA guidelines checklist.
|
Section and Topic |
Item # |
Checklist item |
Location where item is reported (Lines) |
|
TITLE |
|
||
|
Title |
1 |
Identify the report as a systematic review. |
1-2 |
|
ABSTRACT |
|
||
|
Abstract |
2 |
See the PRISMA 2020 for Abstracts checklist. |
6-11 |
|
INTRODUCTION |
|
||
|
Rationale |
3 |
Describe the rationale for the review in the context of existing knowledge. |
34-60 |
|
Objectives |
4 |
Provide an explicit statement of the objective(s) or question(s) the review addresses. |
62-71 |
|
METHODS |
|
||
|
Eligibility criteria |
5 |
Specify the inclusion and exclusion criteria for the review and how studies were grouped for the syntheses. |
85-90 |
|
Information sources |
6 |
Specify all databases, registers, websites, organisations, reference lists and other sources searched or consulted to identify studies. Specify the date when each source was last searched or consulted. |
78-79 |
|
Search strategy |
7 |
Present the full search strategies for all databases, registers and websites, including any filters and limits used. |
79-81 |
|
Selection process |
8 |
Specify the methods used to decide whether a study met the inclusion criteria of the review, including how many reviewers screened each record and each report retrieved, whether they worked independently, and if applicable, details of automation tools used in the process. |
94-121 |
|
Data collection process |
9 |
Specify the methods used to collect data from reports, including how many reviewers collected data from each report, whether they worked independently, any processes for obtaining or confirming data from study investigators, and if applicable, details of automation tools used in the process. |
94-121 |
|
Data items |
10a |
List and define all outcomes for which data were sought. Specify whether all results that were compatible with each outcome domain in each study were sought (e.g. for all measures, time points, analyses), and if not, the methods used to decide which results to collect. |
94-121 |
|
10b |
List and define all other variables for which data were sought (e.g. participant and intervention characteristics, funding sources). Describe any assumptions made about any missing or unclear information. |
99-121 |
|
|
Study risk of bias assessment |
11 |
Specify the methods used to assess risk of bias in the included studies, including details of the tool(s) used, how many reviewers assessed each study and whether they worked independently, and if applicable, details of automation tools used in the process. |
125-131 |
|
Effect measures |
12 |
Specify for each outcome the effect measure(s) (e.g. risk ratio, mean difference) used in the synthesis or presentation of results. |
99-105 |
|
Synthesis methods |
13a |
Describe the processes used to decide which studies were eligible for each synthesis (e.g. tabulating the study intervention characteristics and comparing against the planned groups for each synthesis (item #5)). |
94-121 |
|
13b |
Describe any methods required to prepare the data for presentation or synthesis, such as handling of missing summary statistics, or data conversions. |
99-121 |
|
|
13c |
Describe any methods used to tabulate or visually display results of individual studies and syntheses. |
99-121, 137-172 |
|
|
13d |
Describe any methods used to synthesize results and provide a rationale for the choice(s). If meta-analysis was performed, describe the model(s), method(s) to identify the presence and extent of statistical heterogeneity, and software package(s) used. |
99, 125-126 |
|
|
13e |
Describe any methods used to explore possible causes of heterogeneity among study results (e.g. subgroup analysis, meta-regression). |
107-121 |
|
|
13f |
Describe any sensitivity analyses conducted to assess robustness of the synthesized results. |
109-113, 117-121, 129-131 |
|
|
Reporting bias assessment |
14 |
Describe any methods used to assess risk of bias due to missing results in a synthesis (arising from reporting biases). |
125-131 |
|
Certainty assessment |
15 |
Describe any methods used to assess certainty (or confidence) in the body of evidence for an outcome. |
99 |
|
RESULTS |
|
||
|
Study selection |
16a |
Describe the results of the search and selection process, from the number of records identified in the search to the number of studies included in the review, ideally using a flow diagram. |
137-138, 297 |
|
16b |
Cite studies that might appear to meet the inclusion criteria, but which were excluded, and explain why they were excluded. |
137-138, 297 |
|
|
Study characteristics |
17 |
Cite each included study and present its characteristics. |
328 |
|
Risk of bias in studies |
18 |
Present assessments of risk of bias for each included study. |
169-172, 308 |
|
Results of individual studies |
19 |
For all outcomes, present, for each study: (a) summary statistics for each group (where appropriate) and (b) an effect estimate and its precision (e.g. confidence/credible interval), ideally using structured tables or plots. |
N/A |
|
Results of syntheses |
20a |
For each synthesis, briefly summarise the characteristics and risk of bias among contributing studies. |
137-165, 308 |
|
20b |
Present results of all statistical syntheses conducted. If meta-analysis was done, present for each the summary estimate and its precision (e.g. confidence/credible interval) and measures of statistical heterogeneity. If comparing groups, describe the direction of the effect. |
137-165, 300-306 |
|
|
20c |
Present results of all investigations of possible causes of heterogeneity among study results. |
169-172, 308 |
|
|
20d |
Present results of all sensitivity analyses conducted to assess the robustness of the synthesized results. |
169-172, 308 |
|
|
Reporting biases |
21 |
Present assessments of risk of bias due to missing results (arising from reporting biases) for each synthesis assessed. |
169-172, 308 |
|
Certainty of evidence |
22 |
Present assessments of certainty (or confidence) in the body of evidence for each outcome assessed. |
169-172, 308 |
|
DISCUSSION |
|
||
|
Discussion |
23a |
Provide a general interpretation of the results in the context of other evidence. |
176-260 |
|
23b |
Discuss any limitations of the evidence included in the review. |
262-276 |
|
|
23c |
Discuss any limitations of the review processes used. |
262-276 |
|
|
23d |
Discuss implications of the results for practice, policy, and future research. |
280-287 |
|
|
OTHER INFORMATION |
|
||
|
Registration and protocol |
24a |
Provide registration information for the review, including register name and registration number, or state that the review was not registered. |
78 |
|
24b |
Indicate where the review protocol can be accessed, or state that a protocol was not prepared. |
78 |
|
|
24c |
Describe and explain any amendments to information provided at registration or in the protocol. |
78, N/A |
|
|
Support |
25 |
Describe sources of financial or non-financial support for the review, and the role of the funders or sponsors in the review. |
293-294 |
|
Competing interests |
26 |
Declare any competing interests of review authors. |
292 |
|
Availability of data, code and other materials |
27 |
Report which of the following are publicly available and where they can be found: template data collection forms; data extracted from included studies; data used for all analyses; analytic code; any other materials used in the review. |
336-339 |
Supplementary Table 2: Quantification of sociodemographic variables of interest in the included studies.
|
|
Frequency of Reporting |
Frequency of Analysis |
||||||||||||||
|
Author |
Year |
Country of Origin |
Age |
Sex |
Height |
Weight |
BMI |
Race |
Ethnicity |
Age |
Sex |
Height |
Weight |
BMI |
Race |
Ethnicity |
|
Alter et al.36 |
2017 |
USA |
X |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
Alter et al.37 |
2017 |
USA |
X |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
Badalamente et al.38 |
2015 |
USA |
X |
X |
|
|
|
|
|
X |
X |
|
|
|
|
|
|
Bashir et al.39 |
2015 |
Pakistan |
X |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
Boriani et al.40 |
2017 |
Italy |
X |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
Cantero-Téllez et al.41 |
2015 |
Spain |
X |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
Chung et al.27 |
2019 |
USA |
X |
X |
|
|
|
X |
|
X |
X |
|
|
|
X |
|
|
Curtin et al.28 |
2017 |
USA |
X |
X |
|
|
|
X |
X |
|
|
|
|
|
|
|
|
Dailey et al.42 |
2018 |
USA |
X |
X |
|
|
X |
|
|
|
|
|
|
|
|
|
|
Dale et al.43 |
2020 |
USA |
X |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
De Moraes et al.44 |
2021 |
Brazil |
X |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
Earp et al.45 |
2017 |
USA |
X |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
El-Saeed et al.46 |
2019 |
Egypt |
X |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
Franko et al.47 |
2017 |
USA |
X |
X |
|
|
|
|
|
|
X |
|
|
|
|
|
|
Hansen et al.48 |
2017 |
Denmark |
X |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
Hegazy et al.49 |
2021 |
Saudi Arabia |
X |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
Hutchison et al.50 |
2018 |
USA |
X |
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
Ilyas et al.51 |
2018 |
USA |
X |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
Keulen et al.52 |
2018 |
USA |
X |
X |
|
|
|
X |
|
|
|
|
|
|
|
|
|
Kleiss et al.53 |
2020 |
USA |
X |
X |
|
|
|
X |
|
X |
X |
|
|
|
X |
|
|
Landgren et al.54 |
2017 |
Sweden |
X |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
Logli et al.55 |
2018 |
USA |
X |
X |
|
|
X |
|
|
|
|
|
|
|
|
|
|
Marks et al.56 |
2017 |
Switzerland |
X |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
Martínez-Catalán et al.57 |
2020 |
Spain |
X |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
Nishiwaki et al.58 |
2021 |
Japan |
X |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
Plate et al.59 |
2015 |
USA |
X |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
Roe et al.60 |
2021 |
USA |
X |
X |
|
|
|
X |
X |
|
|
|
|
|
|
|
|
Roh et al.61 |
2015 |
South Korea |
X |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
Roh et al.62 |
2019 |
South Korea |
X |
X |
|
|
X |
|
|
|
|
|
|
|
|
|
|
Saving et al.63 |
2019 |
Sweden |
X |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
Schwartzenberger et al.64 |
2017 |
USA |
X |
X |
|
|
|
|
|
X |
X |
|
|
|
|
|
|
Selles et al.65 |
2020 |
Netherlands |
X |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
Skov et al.30 |
2017 |
Denmark |
X |
X |
|
|
|
|
X |
|
|
|
|
|
|
|
|
Soberón et al.66 |
2016 |
USA |
X |
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
Sørensen et al.67 |
2020 |
Denmark |
X |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
Spekreijse et al.68 |
2015 |
Netherlands |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Strömberg et al.67 |
2016 |
Sweden |
X |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
Tsolias et al.69 |
2018 |
Belgium |
X |
X |
X |
X |
|
|
|
|
|
|
|
|
|
|
|
Tyser et al.22 |
2015 |
USA |
X |
X |
|
|
|
X |
|
X |
X |
|
|
|
|
|
|
Valdes et al.70 |
2015 |
USA |
X |
X |
|
|
|
|
|
X |
|
|
|
|
|
|
|
Wasterlain et al.71 |
2017 |
USA |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Weinheimer et al.72 |
2019 |
USA |
X |
X |
|
|
X |
|
|
|
|
|
|
|
|
|
|
Wilkens et al.73 |
2018 |
USA |
X |
X |
|
|
|
X |
|
|
|
|
|
|
|
|
|
Williksen et al.74 |
2015 |
Norway |
X |
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
Zhuang et al.75 |
2020 |
USA |
X |
X |
|
|
|
X |
X |
X |
|
|
|
|
|
|
|
|
Total |
Count |
44 |
41 |
1 |
1 |
5 |
8 |
4 |
8 |
6 |
0 |
0 |
0 |
2 |
0 |
|
|
% |
97.80% |
91.10% |
2.20% |
2.20% |
11.10% |
17.80% |
8.90% |
17.80% |
13.30% |
0.00% |
0.00% |
0.00% |
4.40% |
0.00% |
|
“X” indicates presence of the indicated variable.
Supplementary Table 3: Proportion of studies reporting sociodemographic variables by year.
|
Year |
Age |
Sex |
BMI |
Race |
Ethnicity |
|
2015 |
100.0% |
88.9% |
0.0% |
11.1% |
0.0% |
|
2016 |
100.0% |
50.0% |
50.0% |
0.0% |
0.0% |
|
2017 |
91.7% |
91.7% |
0.0% |
8.3% |
16.7% |
|
2018 |
100.0% |
85.7% |
28.6% |
28.6% |
0.0% |
|
2019 |
100.0% |
100.0% |
40.0% |
20.0% |
0.0% |
|
2020 |
100.0% |
100.0% |
0.0% |
33.3% |
16.7% |
|
2021 |
100.0% |
100.0% |
0.0% |
25.0% |
25.0% |
Supplementary Table 4: Proportion of studies analyzing sociodemographic variables by year.
|
Year |
Age |
Sex |
BMI |
Race |
Ethnicity |
|
2015 |
33.3% |
22.2% |
0.0% |
0.0% |
0.0% |
|
2016 |
0.0% |
0.0% |
0.0% |
0.0% |
0.0% |
|
2017 |
8.3% |
16.7% |
0.0% |
0.0% |
0.0% |
|
2018 |
14.3% |
0.0% |
0.0% |
0.0% |
0.0% |
|
2019 |
20.0% |
20.0% |
0.0% |
20.0% |
0.0% |
|
2020 |
33.3% |
16.7% |
0.0% |
16.7% |
0.0% |
|
2021 |
0.0% |
0.0% |
0.0% |
0.0% |
0.0% |
Supplementary Table 5: Data for provided figures
a) RCT Country of Origin data.
b) RCT Year of Publication data.
c) Sociodemographic variable reporting.
d) Sociodemographic variable analyzing.
a)
|
Countries |
Count |
|
USA |
24 |
|
Denmark |
3 |
|
Sweden |
3 |
|
Netherlands |
2 |
|
South Korea |
2 |
|
Spain |
2 |
|
Belgium |
1 |
|
Brazil |
1 |
|
Egypt |
1 |
|
Italy |
1 |
|
Japan |
1 |
|
Norway |
1 |
|
Pakistan |
1 |
|
Saudi Arabia |
1 |
|
Switzerland |
1 |
b)
|
Years |
Count |
|
2015 |
10 |
|
2016 |
2 |
|
2017 |
12 |
|
2018 |
7 |
|
2019 |
4 |
|
2020 |
6 |
|
2021 |
4 |
C)
|
Sociodemographic Reporting |
|||||
|
|
Age |
Sex |
BMI |
Race |
Ethnicity |
|
2015 |
9 |
8 |
0 |
1 |
0 |
|
2016 |
2 |
1 |
1 |
0 |
0 |
|
2017 |
11 |
11 |
0 |
1 |
2 |
|
2018 |
7 |
6 |
2 |
2 |
0 |
|
2019 |
5 |
5 |
2 |
1 |
0 |
|
2020 |
6 |
6 |
0 |
2 |
1 |
|
2021 |
4 |
4 |
0 |
1 |
1 |
d)
|
Sociodemographic Analysis |
|||||
|
|
Age |
Sex |
BMI |
Race |
Ethnicity |
|
2015 |
3 |
2 |
0 |
0 |
0 |
|
2016 |
0 |
0 |
0 |
0 |
0 |
|
2017 |
1 |
2 |
0 |
0 |
0 |
|
2018 |
1 |
0 |
0 |
0 |
0 |
|
2019 |
1 |
1 |
0 |
1 |
0 |
|
2020 |
2 |
1 |
0 |
1 |
0 |
|
2021 |
0 |
0 |
0 |
0 |
0 |