
Combining All Available Clinical Outcomes on Cervical Disc Arthroplasty: A Systematic Review and Meta-Analysis
Jenna M. Wahbeh1,2, Claire J. Bogosian1,3, Natalie M. Kistler1,4, Sang-Hyun Park1,5, Edward Ebramzadeh1,4,5, Sophia N. Sangiorgio1,2,5*
1The J. Vernon Luck, Sr., M.D. Orthopaedic Research Center, Orthopaedic Institute for Children in Alliance with UCLA, Los Angeles, CA, USA
2Department of Bioengineering, University of California, Los Angeles, CA, USA
3Department of Bioengineering, University of California, Berkeley, CA, USA
4Department of Biomedical Engineering, University of Southern California, Los Angeles, CA, USA
5Department of Orthopaedic Surgery, University of California, Los Angeles, CA, USA
Abstract
Background: Reviews of total disc arthroplasty (TDA) performance have focused on prospective randomized controlled trials (RCTs), excluding potentially important clinical information reported by others. The goal of the present study was to perform a comprehensive review, including both RCTs and non-randomized cohorts with more than five years of clinical outcome. We further explored the differences in outcome between prospective RCT and non-randomized, including retrospective studies.
Methods: A systematic literature review was performed following PRISMA guidelines. Inclusion criteria were: clinical follow-up ≥ 5 years with quantitative clinical and radiographic outcome. All studies that met these criteria, including retrospective and non-randomized studies, were included, for a total of 62 studies. As anterior cervical discectomies and fusion (ACDF) was included as a control group in the majority of the studies, comparisons between TDA and ACDF were conducted.
Results: Overall, there was a statistically significant difference between the rates of secondary surgeries reported for prospective RCTs and all other studies, with reoperation rates of 5.4% for prospective RCT studies v. 7.5% in all others (P<0.01). Including all studies, the reoperation rate for TDA patients was 5.6% and for fusion patients (included as control groups), 7.8%, (P=0.06). Overall, the reported incidence of adjacent segment degeneration was 26.2% in TDA patients and 43.9% in fusion patients (P<0.001).
Conclusions: These findings demonstrated the need for including all available data to assess the current outcomes of cervical disc arthroplasty and account for potential biases.
Introduction
Total disc arthroplasty (TDA) for the cervical spine was introduced with the promise of preservation of motion and alleviation of pain, while minimizing the likelihood of developing adjacent segment degeneration, a common complication following anterior cervical discectomy and fusion1-3. Given that TDA is still a relatively new technology, long-term outcome studies are necessary to understand the overall clinical performance. Several reviews have reported short-term success for a variety of cervical TDA4-7. Further, some recent studies have presented the combined findings for longer outcomes, ranging from 4-10 years; however, these studies have included only prospective randomized controlled trials (RCT), typically funded by industry, excluding data from thousands of patients in dozens of articles, reported in retrospective and non-randomized studies8-11.
While randomized controlled trials are generally considered to be the most objective way to evaluate an intervention, relying only on these studies may severely compromise, if not bias, a systematic review12. Further, as most RCTs are conducted for regulatory approval, patient selection and inclusion tends to be carefully monitored. This is due largely to the fact that RCTs are costly, limiting clinical trials to large academic centers, typically with substantial industry support. Consequently, the largest of previous published systematic reviews included data from only eleven centers, while clinical use, particularly in the global setting, has become far more widespread9.
In the present study, we provide a comprehensive overview of all available quantitative outcome data for cervical TDA patients with more than five years of follow-up. The goals were to 1) to compare outcomes between randomized and non-randomized studies and 2) combine the outcome of all studies, regardless of whether they were randomized. Accordingly, we expanded the inclusion criteria used previously in other studies by including non-randomized prospective studies, retrospective radiographic reviews, and registry data, to gain a more balanced global perspective on the experience to date with cervical arthroplasty. Outcome variables included: reoperation rates, adjacent segment degeneration, heterotopic ossification, range of motion, and clinical outcome scores.
Methods
Literature Search and Selection Criteria
Two of the authors (C.J.B. and J.M.W.) systematically searched electronic databases following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for this study between June and September 202013. A comprehensive search of the PubMed, Google Scholar, and Medline databases was conducted for studies related to TDA. The keyword search terms used were “cervical disc replacement/arthroplasty,” “long-term outcome,” “radiographic,” “reoperation,” “heterotopic ossification,” or “adjacent segment degeneration”. As adjacent segment degeneration and heterotopic ossification have been heavily studied and commonly reported in current TDA literature, these were included in the search terms, as well.
To be eligible for the systematic review the articles had to: 1) have follow-up data at ≥ 5 years for TDAs, 2) have data for reoperation rates, and partial or complete data for the following: range of motion in flexion/extension (ROM), adjacent segment degeneration (ASD), heterotopic ossification (HO), and/or clinical outcome scores, 3) use radiographic images to quantify ROM, ASD, and/or HO.
Data Extraction
The following categories of data were extracted from each article that met the criteria: 1) general information such as author, date, type of study, number of participants, follow-up rate, device type, and distribution of surgical level, 2) data on experimental design such as key methods and inclusion/exclusion criteria, 3) overall outcome such as reoperation rates, ROM, ASD, HO, as well as any clinical outcome scores, adverse events, and histopathology.
Single-level only studies generally reported index-level and full cervical spine ROM (cROM). Multiple/unspecified level studies reported superior and inferior level ROM as well as cROM. The majority of studies classified HO according to the McAfee classification which uses a scale from 0-4 with grade 0 being no HO and grade 4 being extreme with a spontaneous fusion and complete loss of mobility14.
Statistical Analysis
Incidence rates for dichotomous variables such as adjacent segment degeneration reoperations were calculated using the patient population size of each as a fixed variable in the JBI System for Unified Management, Assessment and Review of Information Software Version 5.0 (JBI, Adelaide, Australia). Odds ratios, and 95% confidence intervals were calculated for these variables using the Mantel-Haenzel statistical method in the JBI Software, as well.
For remaining comparisons, preoperative and postoperative weighted averages were calculated using the number of patients reported and their respective average value, then combining those values and taking the overall average with the total patients, using SPSS Version 19.0 (IBM, Inc., Houston, Texas). Preoperative averages used the number of patients at the beginning of the experiment while postoperative values were taken using the number of patients at the final follow-up based on the follow-up rate reported. Duplicate studies were noted and the study with the longest follow-up time was included in the data analyses, excluding the duplicate. All studies that included a control used ACDF patients as a control group, so this was included throughout the analyses. Comparisons in this review were analyzed using either a Fisher exact test for categorical variables or a t-test for continuous variables.
Results
Included Studies
Over 14,000 articles were initially identified, with the majority of articles, 12,400, being from Google Scholar, then about 2,000 from Medline, and about 600 from PubMed. After the titles were screened to remove duplicates and abstracts were reviewed, 247 articles were identified as possible clinical TDA studies. From these, 164 were removed due to having follow-up periods shorter than 5 years. Then, 21 articles were removed due to lack of data on quantitative outcomes such as adjacent segment degeneration, heterotopic ossification, reoperation rates, or being a case study. This left a total of 62 articles to be reviewed in the present study (Figure 1)1,2,15-73.
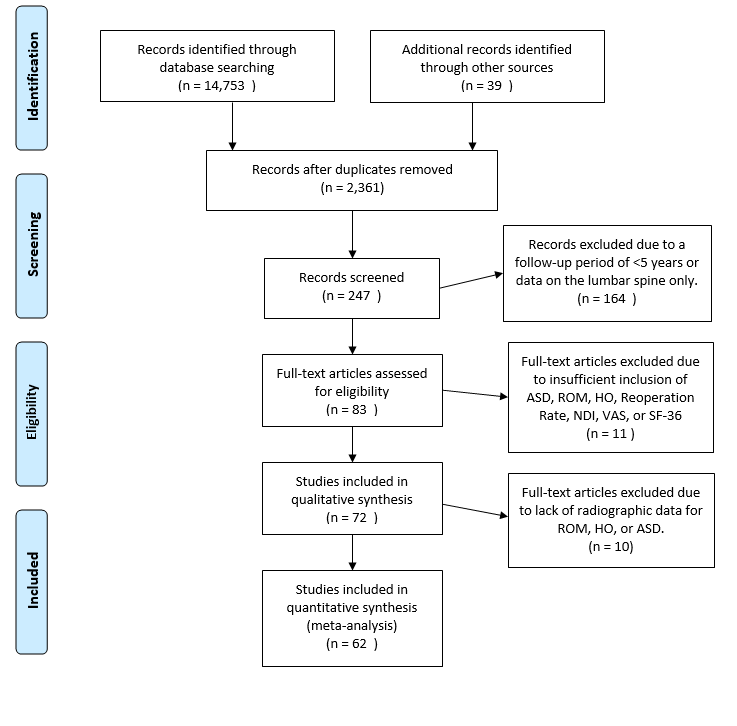
Figure 1: PRISMA diagram outlining the flow of information and selection process for this meta-analysis.
Study characteristics
The literature identified included prospective randomized and nonrandomized controlled trials, comparative studies, retrospective studies, and blinded and unblinded studies (Table 1). Common patient inclusion criteria included degenerative disc disease, radiculopathy, myelopathy, and failed response to non-operative treatment. Common exclusion criteria were multi-level surgery, immobility, or prior cervical spine surgery.
All articles reported on one or more of the following outcome variables: reoperation rates, ROM, ASD, HO, or clinical outcome scores. All other articles were long-term radiographic reviews, with follow-up from 5 to 30 years. The age in individual studies ranged from 35 to 57. The combined mean age was 45.2 ± 5.3 for the TDA group and 48.4 ± 3.5 for the ACDF group, with the majority of the studies age-matched.
Overall, 7,910 patients received a TDA and 8,353 patients received an ACDF that were included in this analysis. Twenty-eight of the included studies were prospective RCTs and the remaining forty were not randomized and included retrospective, and non-randomized studies (Table 1). For brevity and clarity, all prospective RCT studies will be referred to as randomized studies and all other studies will be referred to as nonrandomized studies throughout the remainder of this paper. All 62 studies included data on TDA1,2,15-65 and 33 studies included data on ACDF (Table 1). A total of 50 articles specified the level operated on. The most common level for both TDA and ACDF was C5/C6 at 51% for TDA and 50% for ACDF. The second most levels treated were C6/C7 at 34% for TDA and 35% for ACDF. Therefore, the majority of data presented is known to pertain to treatment at those two levels.
Table 1: Study Characteristics
|
Author, yr |
Study design |
Patients, n |
Mean age (SD), yrs |
Industry Funded (y/n) |
Population pathology |
Investigational Treatment (Type of TDR) |
Control Treatment |
Treatment Level |
Follow-up, yrs |
Follow-up rate (%) |
||||
|
|
|
Total |
Investigational |
Control |
TDR |
ACDF |
|
|
|
|
|
|
TDR |
ACDF |
|
Coric et al., 2018 |
Prospective RCT |
269 |
136 |
133 |
N/A |
N/A |
Y |
Radiculopathy |
Kineflex-C |
ACDF |
1 |
5 |
68.4 |
62.4 |
|
Gao et al., 2018 |
Comparative |
60 |
24 |
36 |
54.7 (6.6) |
58.6 (9.5) |
N |
Radiculopathy and/or myelopathy |
Prestige LP |
ACDF |
2 |
5 |
100 |
100 |
|
Vaccaro et al., 2018 |
Prospective RCT |
346 |
226 |
120 |
41.6 (8.13)*, 43.3 (7.5)** |
44.4 (7.86) |
Y |
Radiculopathy and/or myelopathy |
Secure-C |
ACDF |
1 |
7 |
81.9 |
84.2 |
|
Mehren et al., 2017 |
Nonrandomized study |
50 |
50 |
N/A |
44.8 (N/A) |
N/A |
N |
Radiculopathy |
ProDisc-C |
N/A |
1,2,3 |
10 |
80.8 |
N/A |
|
Phillips et al., 2015 |
Prospective RCT |
403 |
218 |
185 |
N/A |
N/A |
Y |
Radiculopathy and/or myelopathy |
PCM |
ACDF |
1 |
7 |
74.8 |
70.3 |
|
Burkus et al., 2014 |
Prospective RCT |
541 |
276 |
265 |
43.3 |
43.9 |
Y |
Radiculpathy |
Prestige LP |
ACDF |
1 |
7 |
76.8 |
69.1 |
|
Lanman et al., 2017 |
Prospective RCT |
397 |
209 |
188 |
47.1 (8.3) |
47.3 (7.7) |
Y |
Radiculopathy and/or myelopathy |
Prestige LP |
ACDF |
2 |
7 |
76.2 |
74.1 |
|
Radcliff et al., 2017, 1 level |
Prospective RCT |
575 |
164 |
81 |
43.3 (9.2) |
44 (8.2) |
Y |
Radiculopathy and/or myelopathy |
Mobi-C |
ACDF |
1 |
7 |
80.1 |
74.3 |
|
Radcliff et al., 2017 2 level |
Prospective RCT |
330 |
225 |
105 |
45.3 (8.1) |
46.2 (8) |
Y |
Radiculopathy and/or myelopathy |
Mobi-C |
ACDF |
2 |
7 |
84.4 |
75 |
|
Janssen et al., 2015 |
Prospective RCT |
209 |
103 |
106 |
43.5 (8.42) |
43.5 (7.15) |
Y |
Radiculopathy |
ProDisc-C |
ACDF |
1 |
7 |
91.9 |
92.4 |
|
Aghayev et al., 2013 |
Retrospective registry search |
332 |
332 |
N/A |
N/A |
N/A |
N |
N/A |
Bryan, Prestige LP, Discover, Mobi-C, and ProDisc-C |
N/A |
2 |
5 |
72.7 |
N/A |
|
Park et al., 2012 |
Retrospective cross-sectional study |
43 |
22 |
21 |
39.9 |
44.3 |
N |
Radiculopathy |
ProDisc-C |
ACDF |
1 |
5 |
100 |
100 |
|
Coric et al., 2013 |
Prospective RCT |
74 |
41 |
33 |
49.5 |
49.3 |
Y |
Radiculopathy |
Bryan and Kineflex-C |
ACDF |
1 |
9 |
86.3 |
86.3 |
|
Zeng et al., 2018 |
Retrospective |
78 |
78 |
N/A |
44.1 (6.7) |
N/A |
N |
Radiculopathy and/or myelopathy |
Not mentioned |
N/A |
1,2 |
9 |
78.2 |
N/A |
|
Lei et al., 2016 |
Prospective, nonrandomzied |
97 |
42 |
55 |
42.6 (6.3) |
47.7 (7.2) |
N |
Radiculopathy or myelopathy |
Bryan |
ACDF |
1 |
8 |
73.8 |
63.6 |
|
Song et al., 2018 |
Prospective nonrandomized |
91 |
91 |
N/A |
55.69 (8.32) |
N/A |
N |
Radiculopathy and/or myelopathy |
Bryan Disc |
N/A |
1 |
10 |
78 |
N/A |
|
Guo et al., 2020 |
Retrospective contrast study |
113 |
47 |
66 |
42.9 (6.3) |
49.38 (9.89) |
N |
N/A |
ProDisc-C |
ACDF |
1 |
8 |
100 |
100 |
|
Yang et al., 2014 |
Retrospective case series study |
37 |
37 |
N/A |
38 |
N/A |
N |
Radiculopathy and/or myelopathy |
Unnamed artificial cervical disk |
N/A |
1,2 |
33 |
56.76 |
N/A |
|
Dufour et al., 2019 |
Prospective nonrandomized |
384 |
384 |
N/A |
44.8 (8.1) |
N/A |
Y |
Radiculopathy and/or myelopathy |
Mobi-C |
N/A |
1,2,3,4 |
5 |
80.6 |
N/A |
|
Tian et al., 2017 |
Prospective nonrandomized |
93 |
45 |
48 |
45 |
48.7 |
N |
Radiculopathy and/or myelopathy |
Bryan |
ACDF |
1,2 |
8.33 |
62.2 |
72.9 |
|
Radcliff et al., 2016 |
Prospective RCT |
330 |
225 |
105 |
45.3 (8.1) |
46.2 (7.99) |
Y |
Radiculopathy or myelopathy |
Mobi-C |
ACDF |
2 |
5 |
90.7 |
86.7 |
|
Burkus et al., 2010 |
Prospective, nonrandomized |
541 |
276 |
265 |
43.3 |
43.9 |
Y |
Radiculopathy or myelopathy |
Prestige LP |
ACDF |
1 |
5 |
52.2 |
47.9 |
|
Cao et al., 2015 |
Prospective RCT |
120 |
60 |
60 |
41 |
44 |
N |
Radiculopathy or myelopathy |
Bryan |
ACDF |
1 |
5 |
100 |
100 |
|
Hisey et al., 2016 |
Prospective RCT |
245 |
164 |
81 |
N/A |
N/A |
Y |
Radiculopathy or myelopathy |
Mobi-C |
ACDF |
1 |
5 |
85.5 |
78.9 |
|
Delamarter et al., 2013 |
Prospective RCT |
209 |
103 |
106 |
N/A |
N/A |
Y |
Radiculopathy |
ProDisc-C |
ACDF |
1 |
5 |
72.7 |
63.5 |
|
Sasso et al., 2017 |
Prospective RCT |
47 |
22 |
25 |
N/A |
N/A |
Y |
Radiculopathy or myelopathy |
Bryan Disc |
ACDF |
1 |
10 |
86.4 |
92 |
|
Zhao et al., 2010 |
Prospective nonrandomized |
22 |
22 |
N/A |
43.8 |
N/A |
N |
Radiculopathy and/or myelopathy |
Bryan Disc |
N/A |
1,2 |
5.75 |
100 |
N/A |
|
Loumeau et al., 2016 |
Prospective RCT |
44 |
22 |
22 |
N/A |
N/A |
Y |
Radiculopathy and/or myelopathy |
ProDisc-C |
ACDF |
1 |
7 |
34 |
86 |
|
Zigler et al., 2013 |
Prospective RCT |
209 |
103 |
106 |
42.1 (8.4) |
43.5 (7.1) |
Y |
Radiculopathy |
ProDisc-C |
ACDF |
1 |
5 |
72.7 |
63.5 |
|
Gornet et al., 2016 |
Prospective nonrandomized (TDR) retrospective analysis for control (ACDF) |
545 |
280 |
265 |
44.5 (8.8) |
43.9 (8.8) |
Y |
Radiculopathy and/or myelopathy |
Prestige LP |
ACDF |
1 |
7 |
75.9 |
70 |
|
MacDowall et al., 2019 |
Register-Based cohort study (nonrandomized) |
3998 |
204 |
3794 |
46.4 (8.2) |
49.9 (9.2) |
Y |
Radiculopathy |
Bryan, ProDisc-C, Discover, Prestige LP, Baguera, Kineflex-C |
ACDF |
N/A |
10 |
40.7 |
32.7 |
|
Han et al., 2019 |
Prospective nonrandomized |
85 |
85 |
N/A |
55.9 (7.9) |
N/A |
N |
Radiculopathy or myelopathy |
Bryan Disc |
N/A |
1 |
10.75 |
77.6 |
N/A |
|
Su Kim et al., 2016 |
Prospective Clinical Study nonrandomzied |
23 |
23 |
N/A |
45 |
N/A |
N |
N/A |
ProDisc-C |
N/A |
1 |
5 |
100 |
N/A |
|
Sun et al., 2012 |
Radiographic review |
56 |
26 |
30 |
44 |
N/A |
N |
N/A |
Bryan |
ACDF |
1 |
5 |
100 |
80 |
|
Zhao et al., 2016 |
Retrospective |
48 |
48 |
N/A |
44.8 |
N/A |
N |
Radiculopathy or myelopathy |
Bryan |
N/A |
1,2 |
10 |
68.75 |
N/A |
|
Hui et al., 2019 |
Retrospective |
45 |
45 |
N/A |
43.6 (5.9) |
N/A |
N |
Radiculopathy or myelopathy |
Prestige LP |
N/A |
1 |
5 |
93.3 |
N/A |
|
Dejaegher et al., 2016 |
Prospective RCT |
89 |
89 |
N/A |
N/A |
N/A |
Y |
Radiculopathy and/or myelopathy |
Bryan |
N/A |
1 |
10 |
81 |
N/A |
|
Malham et al., 2013 |
Retrospective |
24 |
24 |
N/A |
40.3 (5.9) |
N/A |
N |
Radiculopathy |
ProDisc-C |
N/A |
1,2 |
9 |
79.2 |
N/A |
|
Nunley et al., 2018 1 level split |
Retrospective |
164 |
164 |
N/A |
N/A |
N/A |
Y |
Radiculopathy or myelopathy |
Mobi-C |
N/A |
1 |
7 |
65.9 |
N/A |
|
Nunley et al., 2018 2 level |
Retrospective |
225 |
225 |
N/A |
N/A |
N/A |
Y |
Radiculopathy or myelopathy |
Mobi-C |
N/A |
2 |
7 |
70.2 |
N/A |
|
Quan et al., 2011 |
Retrospective |
21 |
21 |
N/A |
46 |
N/A |
N |
Radiculopathy |
Bryan |
N/A |
1,2 |
8 |
100 |
N/A |
|
Wang et al., 2018 |
Retrospective |
38 |
38 |
N/A |
56.8 |
N/A |
N |
Radiculopathy and/or myelopathy |
DCI |
N/A |
1,2 |
6.5 |
100 |
N/A |
|
Goffin et al., 2010 1 level split |
Prospective RCT |
89 |
89 |
N/A |
43.2 (9) |
N/A |
Y |
Radiculopathy and/or myelopathy |
Bryan |
N/A |
1 |
6 |
100 |
N/A |
|
Goffin et al., 2019 2 level split |
Prospective RCT |
9 |
9 |
N/A |
49.3 (7.2) |
N/A |
Y |
Radiculopathy and/or myelopathy |
Bryan |
N/A |
2 |
6 |
100 |
N/A |
|
Lavelle et al., 2019 |
Prospective RCT |
242 |
221 |
104 |
44.4 |
44.7 |
Y |
Radiculopathy or myelopathy |
Bryan |
ACDF |
1 |
10 |
100 |
100 |
|
Pointillart V et al., 2018 |
Prospective nonrandomized |
21 |
21 |
N/A |
46.2 |
N/A |
N |
Radiculopathy |
Bryan |
N/A |
1,2 |
15 |
85.7 |
N/A |
|
Skeppholm et al., 2017 |
Retrospective, Comparative |
676 |
172 |
504 |
46.6 (4.5) |
47.3 (3.1) |
N |
Radiculopathy |
Discover, Prestige LP |
ACDF |
1,2,3 |
5 |
94 |
94 |
|
Walraevens et al., 2010 |
Prospective nonrandomized |
89 |
89 |
N/A |
42.8 (8) |
N/A |
Y |
Radiculopathy and/or myelopathy |
Bryan Disc |
N/A |
1 |
8 |
29 |
N/A |
|
Zhao et al., 2013 |
Prospective nonrandomzied |
26 |
26 |
N/A |
44 |
N/A |
N |
Radiculopathy or myelopathy |
ProDisc-C |
N/A |
1 |
6.33 |
100 |
N/A |
|
Gornet et al., 2019, 2-level |
Prospective RCT |
266 |
148 |
118 |
47.1 (8.3) |
N/A |
Y |
Radiculopathy or myelopathy |
Prestige LP |
ACDF |
2 |
10 |
86 |
84.9 |
|
Ryu et al., 2013 |
Prospective RCT |
20 |
20 |
N/A |
N/A |
N/A |
N? |
Radiculopathy and/or myelopathy |
Bryan |
N/A |
1 |
5 |
100 |
N/A |
|
Gornet et al., 2019, 1-level |
Prospective nonrandomized |
545 |
280 |
265 |
44.5 (8.8) |
N/A |
Y |
Radiculopathy and/or myelopathy |
Prestige LP |
ACDF |
1 |
10 |
83.3 |
84.9 |
|
Kumar et al., 2020 |
Retrospective Cohort Anlaysis |
670 |
335 |
335 |
45.3 (8) |
51 (10.4) |
N |
Radiculopathy and/or myelopathy |
|
ACDF |
1 |
5 |
100 |
100 |
|
Shang et al., 2017 |
Retrospective |
49 |
18 |
31 |
48.7 (6.1) |
49.3 (8.6) |
N |
Radiculopathy or myelopathy |
Bryan |
ACDF |
1 |
9.17 |
100 |
100 |
|
Yang et al., 2017 |
nonrandomized |
186 |
78 |
108 |
52 (19) |
50 (18) |
N |
Radiculopathy |
Bryan Disc |
ACDF |
1 |
10 |
100 |
100 |
|
Jackson et al., 2016 1 level split |
Prospective RCT |
260 |
179 |
81 |
N/A |
N/A |
Y |
Radiculopathy or myelopathy |
Mobi-C |
ACDF |
1 |
5 |
85.5 |
78.9 |
|
Jackson et al., 2016 2 level split |
Prospective RCT |
339 |
234 |
105 |
N/A |
N/A |
Y |
Radiculopathy or myelopathy |
Mobi-C |
ACDF |
2 |
5 |
90.7 |
86.7 |
|
Zhao et al., 2020 |
Retrospective |
43 |
27 |
16 |
44 |
44 |
N |
Radiculopathy or myelopathy |
ProDisc-C |
ACDF |
1 |
10 |
100 |
69 |
|
Lobo et al., 2020 |
Retrospective |
22 |
22 |
N/A |
39.7 |
N/A |
N |
Degenerative Disc Disease |
Bryan and Prestige |
N/A |
1 |
10 |
68 |
N/A |
|
Zhou et al., 2020 |
Retrospective |
54 |
54 |
N/A |
43.6 |
N/A |
N |
Radiculopathy or myelopathy |
Bryan |
N/A |
1,2,3 |
10 |
100 |
N/A |
|
Cao et al., 2022 |
Retrospective |
28 |
28 |
N/A |
43 |
N/A |
N |
Myelopathy or radiculopathy |
ProDisc-C |
N/A |
1 |
10 |
100 |
N/A |
|
Kim et al., 2021 |
Prospective RCT |
257 |
257 |
N/A |
N/A |
N/A |
Y |
Radiculopathy or myelopathy |
Mobi-C |
N/A |
1,2 |
7 |
81 |
N/A |
|
Genitiempo et al., 2020 |
Retrospective |
103 |
71 |
31 |
42.7 |
42.7 |
N |
Radiculopathy |
Bryan |
ACDF |
1 |
18.8 |
82 |
26 |
|
Ghobrial et al., 2018 |
Prospective RCT |
463 |
242 |
221 |
N/A |
N/A |
Y |
Radiculopathy or myelopathy |
Bryan, Prestige LP |
ACDF |
1 |
10 |
54 |
47 |
|
Nunley et al., 2020 |
Prospective RCT |
575 |
389 |
186 |
N/A |
N/A |
N |
Degenerative Disc Disease |
Mobi-C |
ACDF |
1,2 |
7 |
100 |
100 |
|
Nunley et al., 2020 |
Prospective RCT |
575 |
389 |
186 |
N/A |
N/A |
N |
Degenerative Disc Disease |
Mobi-C |
ACDF |
1,2 |
7 |
100 |
100 |
* = nonrandomized cohort if reported separately, ** = randomized cohort if reported separately, TDR, total disc replacement group; ACDF, anterior cervical discectomy and fusion group; N/A, not available; RCT, randomized controlled trial; SD, standard deviation
Reoperation
Secondary procedures were reported as: reoperation for any reason, reoperation at the index level, reoperation at the adjacent level, removal of the device, revision of the device, or supplemental fixation. All secondary procedure values were statistically different between the randomized studies and the non-randomized studies. Overall secondary surgery was performed in 5.4% of patients in randomized studies (132/ 2,129) and 7.5% of patients in non-randomized studies (74/ 754) (P<0.01). Reoperation at the adjacent level was 4.3% in randomized studies and 6.1% in non-randomized studies (P<0.001). Reoperation at the index level was 2.6% in randomized studies and 4.4% in non-randomized studies (P<0.001) (Figure 2a).
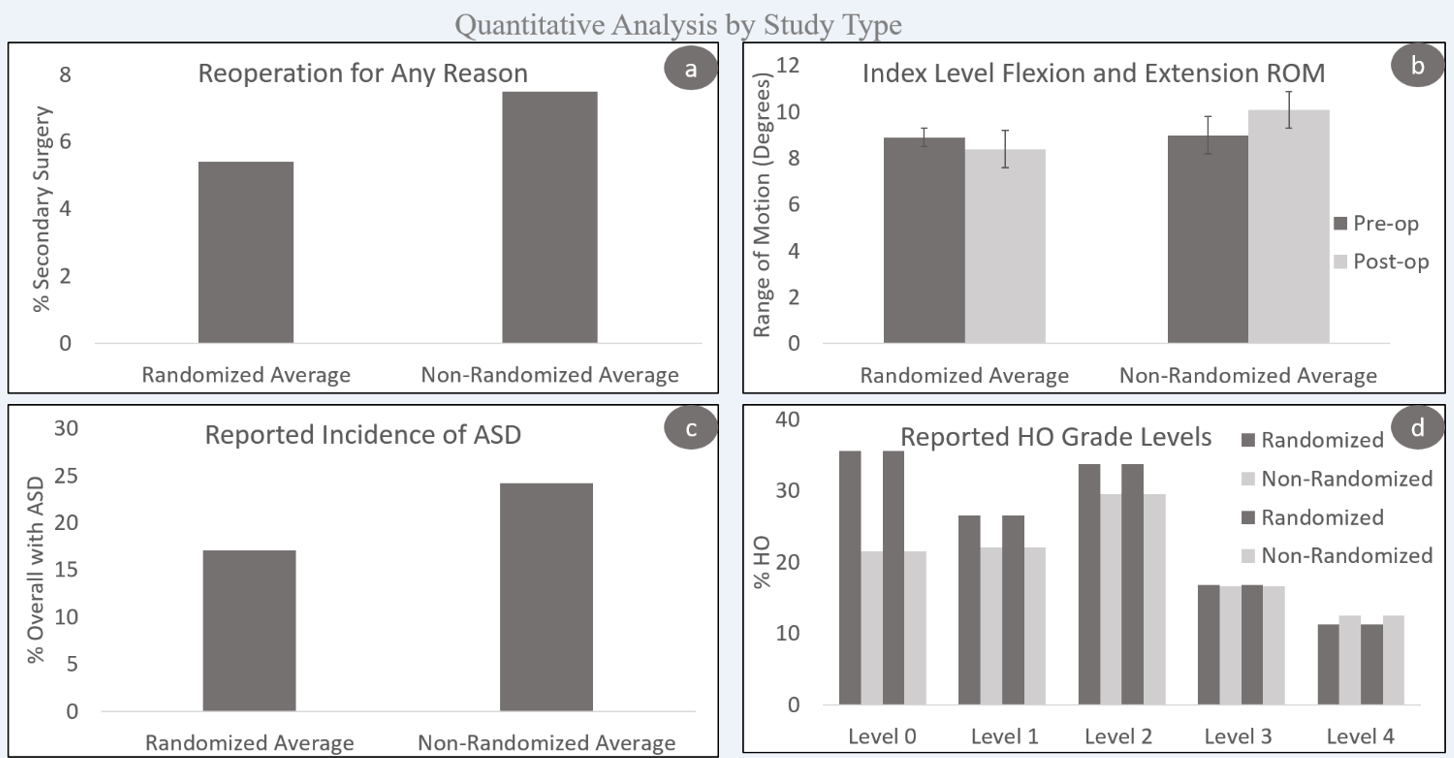
Figure 2: Combined averages of reported quantitative analysis by device type. a) Reoperation for any reason, b) flexion/extension ROM, c) reported incidence of ASD, d) reported incidence of HO present.
The combined rates of reoperation for any reason for TDA patients was 5.6% and for ACDF patients was 7.8% (P=0.06; OR=0.48; CI=0.39, 0.60) (Figure 3). Reoperation was defined as any procedure at the index level or adjacent level that does not remove, modify, or add to the original implant. Removal surgery removed one or all components of the original implant. Revision involved the modification of the original implant without removal. Supplemental fixation occurred if nonunion occurs, typically supplemental fixation is an additional posterior fusion approach. All these secondary procedure rates were reported for TDA and ACDF surgeries (Table 2 and Appendix).
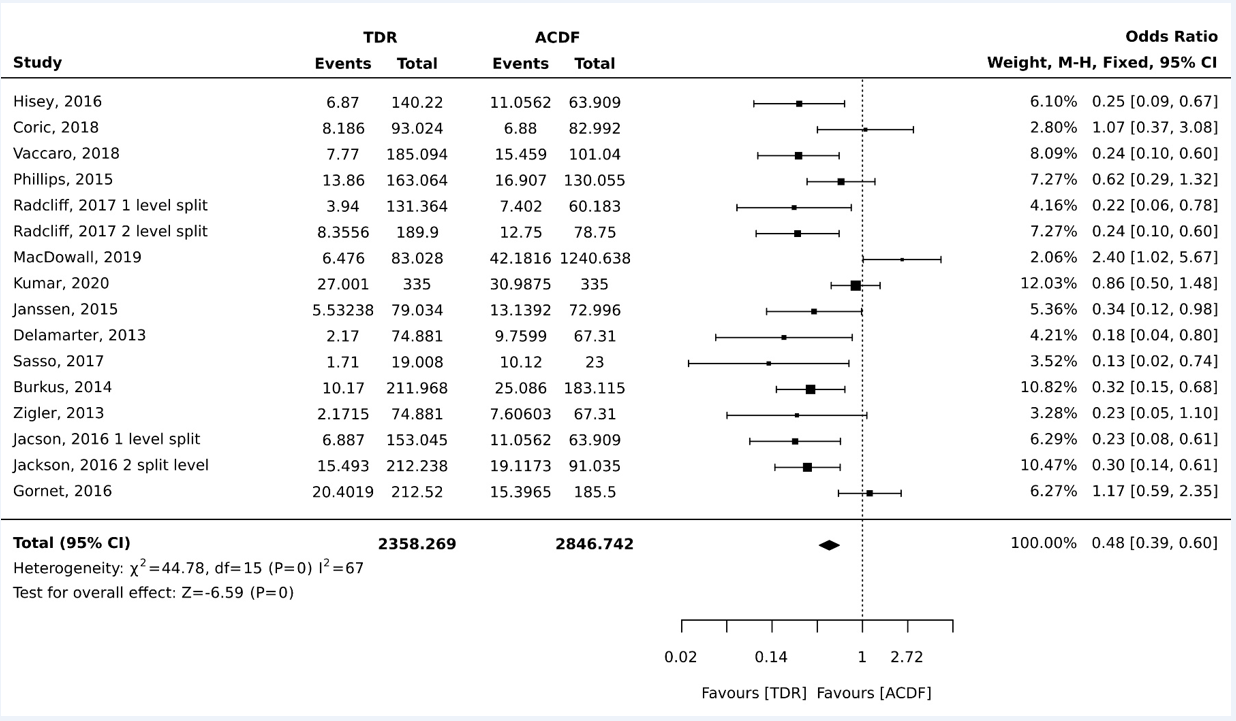
Figure 3: Statistical analysis using JBI software for overall reoperation rates comparing studies with TDR patients and the ACDF control patients.
Table 2: Secondary Surgery Rates
|
|
TDR (%)* |
ACDF (%)* |
P value |
Odds Ratio |
95% Confidence Interval |
|
Overall Rate (no. [%]) |
212/3569 (5.6%) |
412/5946 (7.8%) |
0.06 |
0.48 |
0.39, 0.60 |
|
Index Level |
141/3128 (3.8%) |
290/5942 (5.4%) |
0.47 |
0.55 |
0.43, 0.71 |
|
Adjacent Level |
173/3397 (4.8%) |
321/6037 (5.8%) |
0.67 |
0.50 |
0.39, 0.64 |
|
Removal |
70/2012 (0%) |
65/1275 (4.7%) |
0.04 |
0.78 |
0.51, 1.19 |
|
Revision |
8/1595 (0%) |
25/1194 (1.9%) |
<0.001 |
0.23 |
0.07, 0.8 |
|
Supp. Fixation |
17/1527 (1.5%) |
38/1169 (3%) |
<0.001 |
0.34 |
0.13, 0.86 |
TDR, total disc replacement group; ACDF, anterior cervical discectomy and fusion group; Supp. Fixation, supplemental fixation *Percentages reported with sample size as a fixed variable
Preservation of Motion
The combined average index level preoperative range of motion (ROM) in flexion/extension for randomized studies was 8.9°with a post-op ROM of 8.4°. Non-randomized studies reported an average pre-op ROM at the index level of 9.0° and post-op of 10.0° (P<0.001) (Figure 2b).
Patients with TDA reported an average pre-op ROM at the index level of 7.9°, with a slight decrease following surgery to 7.8° (P<0.001)1,2,15-19,21,22,24-32,34-42,44-47,49-52,54-56,58-61,74,75. As expected, ACDF patients had a preoperative ROM of 7.8° with a postoperative reduction to 0.8° (P<0.001) (Table 3). Of the articles that reported treatment level and were included in the ROM calculations, levels C5/C6 and C6/C7 were the most frequent index level. For TDA patients, 50% of patients had a C5/C6 arthroplasty and 35% of patients had a C6/C7 arthroplasty. These results were mimicked with ACDF patients– 49% of patients had a C5/C6 fusion and 36% of patients had a C6/C7 fusion. The full cervical spine ROM for TDA patients was 43.7° increasing slightly after surgery to 45.1°. For ACDF patients, the full cervical spine ROM was 39.2° decreasing postoperatively to 32.2° (P<0.001).
Table 3: ROM Pre-operative and Post-operative Values for TDR and ACDF at 1- and Multiple/Unspecified Levels
|
|
TDR |
ACDF |
||
|
|
Preop (SD) |
Postop (SD) |
Preop (SD) |
Postop (SD) |
|
Single Level Specified |
|
|
|
|
|
Index/FSU |
7.9 (1.1) |
7.8 (1.6) |
7.8 (0.4) |
0.8 (2.2) |
|
cROM (C2-C7) |
43.7 (4.9) |
45.1 (2.8) |
39.2 (6.5) |
32.2 (5.3) |
|
Multiple Levels |
|
|
|
|
|
Superior |
8.6 (1.5) |
9.4 (2.0) |
10.0 (1.4) |
6.6 (5.3) |
|
Inferior |
7.0 (1.3) |
7.5 (1.1) |
7.4 (1.2) |
5.1 (3.8) |
Adjacent Segment Degeneration
Twenty-six studies included data on adjacent segment degeneration (ASD)17,18,22,24,25,27,29,30,32-37,39,41,44,47-49,52,56,61-64. Among these studies, when randomized and non-randomized studies were compared, the difference in the number of patients with ASD and without ASD was significantly different (P<0.02). Specifically, randomized studies reported the presence of ASD in 17.1% of patients (227/ 1167) and non-randomized studies reported the presence of ASD in 24.2% of patients (265/ 1128) (Figure 2c).
Among these studies TDAs were also compared to ACDF. Overall, the reported incidence of ASD in patients with TDA was 26.2%, and in patients with ACDF was 43.9%, (P<0.01; OR=0.35; CI=0.39,0.64) (Figure 4). While some studies specified the location of ASD as superior and/or inferior, in the present analysis, the location of ASD did not differ widely among TDA patients (superior = 30.6% v. inferior = 30.5%) or among ACDF patients (superior = 68.4% v. inferior = 62.2%) (Table 4).
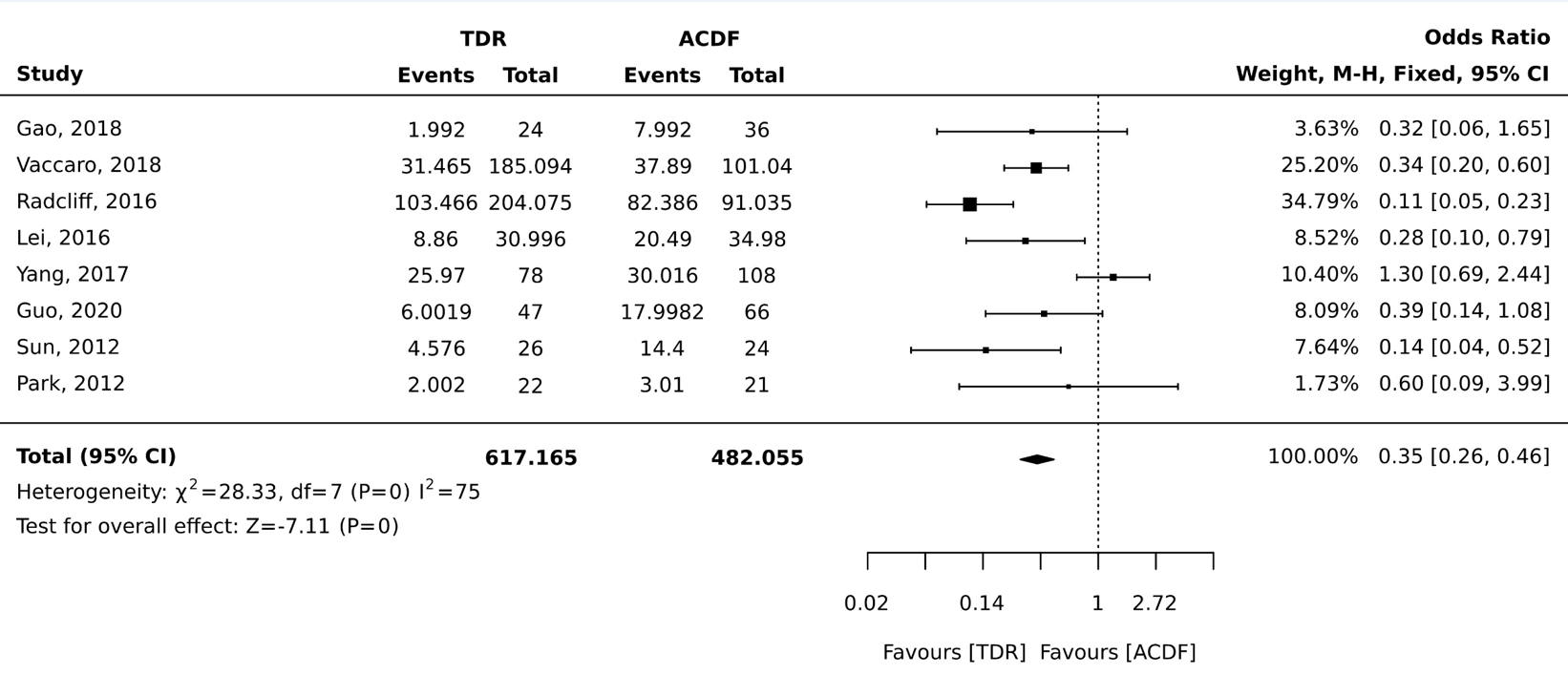
Figure 4: Statistical analysis using JBI software for adjacent segment degeneration comparing studies with TDR patients and the ACDF control patients.
Table 4: Adjacent Segment Degeneration Rates (ASD)
|
|
TDR (%)* |
ACDF (%)* |
P value |
|
Overall Rate (no. [%]) |
374/1352 (26.2%) |
224/513 (43.9%) |
<0.001 |
|
Superior |
524/1643 (30.6%) |
362/542 (68.4%) |
<0.001 |
|
Inferior |
537/1643 (30.5%) |
333/542 (62.2%) |
<0.001 |
TDR, total disc replacement group; ACDF, anterior cervical discectomy and fusion group; *Percentages reported with sample size considered as a fixed variable
Heterotopic Ossification
Incidence of heterotopic ossification (HO) was reported in 34 studies15-19,21,22,24-28,30,32,33,35-37,39,40,44-47,49,50,52,55,58,60,62-64,74. Heterotopic ossification was reported in TDA patients as a grade (0 through 4) according to the McAfee classification system or as absent versus present. When randomized and non-randomized studies were compared, the presence of heterotopic ossification was significantly different (P<0.01). In randomized studies, the absence of HO was reported in 35 patients of 100 (35%) of patients. In non-randomized studies, the absence of HO was reported in 244 patients of 1,133 (21.5%). In randomized studies, in grade 1 HO was reported in 26.5% of patients, grade 2 in 33.8% of patients, grade 3 in 16.8% of patients and grade 4 in 11.3% of patients. In non-randomized studies grade 1 was reported in 22% of patients, grade 2 in 29.5% of patients, grade 3 in 16.6% of patients and grade 4 in 12.5% of patients (Figure 2d). Grade 1 and grade 2 are considered not clinically relevant while grade 4 is a severe, symptomatic presentation of HO.
Including all studies, a total of 2,762 TDA patients had HO reported as absent or present. The HO absence rate was 56.0% (1,548/2,761), meaning a majority of patients did not display signs of HO. The presence of HO was in the minority with a rate of 43.9% (1,211/2,761). A total of 2,271 patients had graded HO reported. The scale most used was the McAfee Classification. Among the rated patients, the incidence of Grade 1 was 6.7% (153/2,271), grade 2 was 14.5% (330/2,271), grade 3 was 13.9% (316/2,271), and grade 4 was 13.8% (313/2,270).
Clinical Outcome
The majority of studies assessed and reported clinical outcome using neck disability index (NDI), visual analog scale (VAS) neck and/or arm pain, SF-36 physical component summary (PCS) or mental component summary (MCS), and Japanese Orthopaedic Association (JOA) scores1,15-19,21,23-30,32,34,35,37-44,46-48,51-56,59-62,64,65,74,76. These are patient-reported outcomes in which patients complete a questionnaire to rank their pain on items such as personal care, lifting, headaches, concentration, etc.
Both randomized and non-randomized studies reported improved clinical outcome scores for NDI, VAS neck and/or arm pain, and SF-36 PCS or MCS (P<0.001). No randomized studies reported JOA scores; therefore, this comparison was not included. Interestingly, all non-randomized studies had lower post-operative scores for NDI and VAS arm/neck than randomized studies (Figure 5). All clinical outcomes improved significantly from baseline in both TDA and ACDF groups (P<0.001) (Table 5).
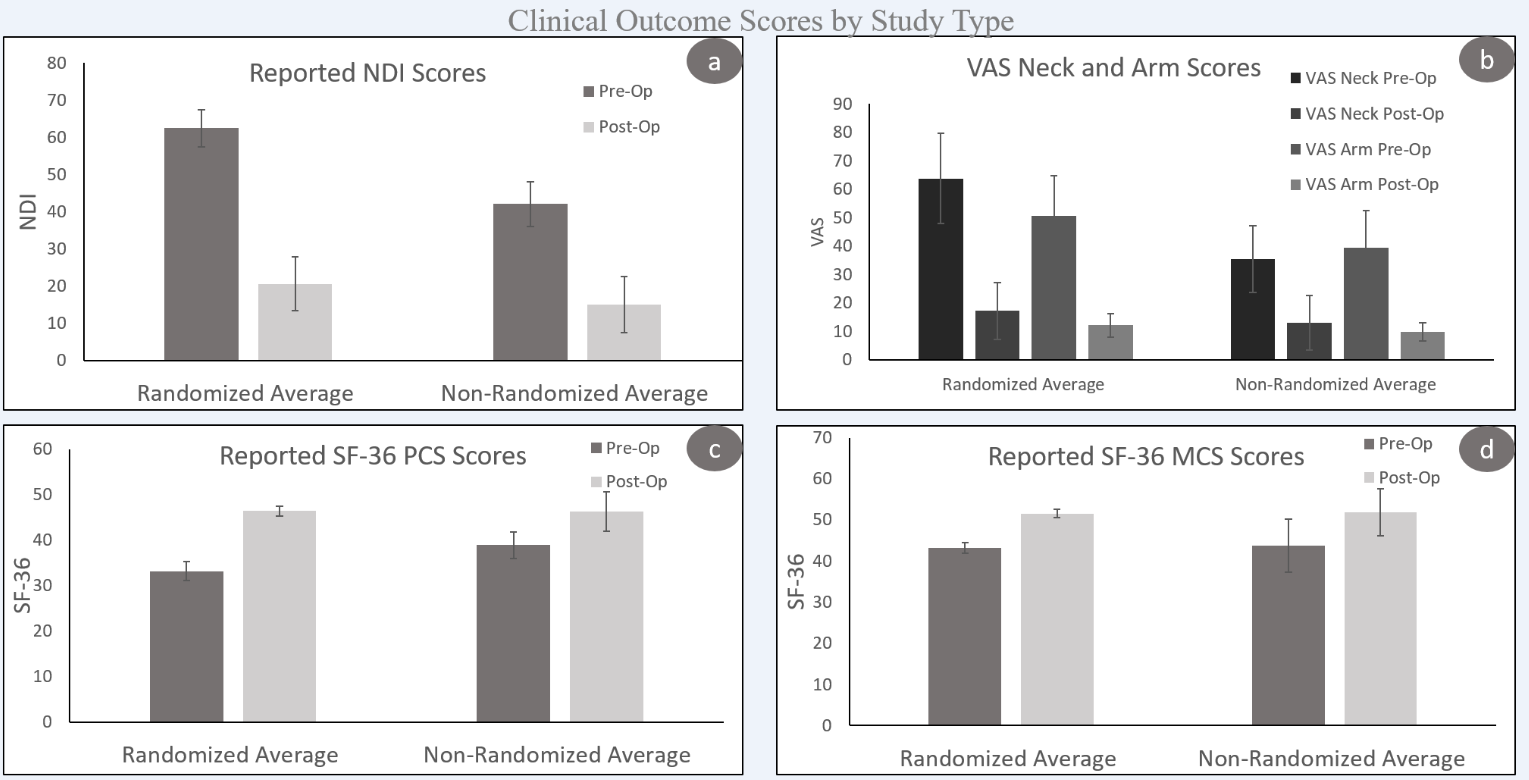
Figure 5: Combined averages of reported clinical outcome scores by device type. a) reported NDI scores, b) reported VAS arm and neck pain scores, c) reported SF-36 PCS scores, d) reported SF-36 MCS scores.
Table 5: Clinical Preoperative and Postoperative Values in both TDR and ACDF patients
|
|
TDR |
ACDF |
P value |
|
NDI scores |
|
|
|
|
Preop (SD) |
52.7 (12.3) |
46.1 (8.8) |
<0.001 |
|
Postop (SD) |
18.7 (12) |
22.4 (5.9) |
<0.001 |
|
VAS neck pain scores (1-10) |
|
|
|
|
Preop (SD) |
6.7 (1.5) |
6.1 (0.9) |
<0.001 |
|
Postop (SD) |
2.2 (1.3) |
2.8 (1.2) |
<0.001 |
|
VAS arm pain scores (1-10) |
|
|
|
|
Preop (SD) |
6.3 (1.2) |
5.9 (1.0) |
<0.001 |
|
Postop (SD) |
2.5 (2.1) |
2.4 (0.7) |
<0.001 |
|
SF-36 PCS |
|
|
|
|
Preop (SD) |
33.4 (1.9) |
32.5 (1.6) |
<0.001 |
|
Postop (SD) |
46.4 (1.7) |
44.1 (1.3) |
<0.001 |
|
SF-36 MCS |
|
|
|
|
Preop (SD) |
41.8 (4.4) |
42.5 (1.5) |
<0.001 |
|
Postop (SD) |
51.0 (3.3) |
49.4 (2.1) |
<0.001 |
|
JOA scores |
|
|
|
|
Preop (SD) |
10.7 (2.0) |
9.7 (1.6) |
<0.001 |
|
Postop (SD) |
15.6 (0.6) |
15.8 (0.4) |
<0.001 |
Discussion
In the present study, the findings from 62 peer-reviewed manuscripts that reported quantitative data with a minimum follow-up of five years were reviewed and evaluated to assess the overall performance of cervical disc arthroplasty to date. In previous systematic reviews of cervical TDA outcome, only randomized controlled trials were included, resulting in a limited and potentially biased scope of investigation. In contrast, in the present study, by including retrospective and non-randomized studies, we were able to include an additional 57 publications, and five-thousand additional patients. A number of articles in the orthopaedic literature as well as other medical subspecialties have addressed the potential limitations and short-comings of including only prospective randomized studies when making evidence-based conclusions12,77-79.
While the results of the present study do not directly contradict previous systematic reviews comparing TDA and ACDF, our study provides original findings in four different aspects of TDA outcome. First, we were able to compare results of the included prospective RCT studies and the remaining non-randomized studies. From this, we showed the importance of utilizing all available data to understand the clinical outcomes of the general population. Additionally, as we intended, we were able to assess TDA outcome at a higher length of follow-up than previous systematic reviews and meta-analyses. Third, our results show a narrower margin of difference in the outcome of patients who were eligible for TDAs, but received either a disc arthroplasty or fusion. Specifically, the rate of secondary surgeries at the index level does not show a significant difference between ACDF and TDA patients. Overall, the success rates in this systematic review show very different results than those of the randomized controlled trials, further validating the need to examine all possible data to gain a broad understanding of implant success in the general population9. Finally, compared to previous publications, the present study provided a more thorough analysis of the specific complications involved in TDA, such as breaking down reoperations into categories and reporting adjacent segment degeneration by the level affected.
Comparison of RCT to other studies
Most outcomes were significantly different between the reported patient averages of randomized studies and non-randomized studies, with major outcomes showing better success in randomized studies. Specifically, the overall variables of most interest to this review that showed differences, favoring randomized studies, were reoperation rates, adjacent segment degeneration, and heterotopic ossification. The grades of HO were varying between being significantly different; however, randomized studies reported more patients with an absence of any HO or with non-clinically relevant HO (grades 1 and 2) and significantly less patients with severe HO, grade 4, than non-randomized studies. Further, all secondary surgery rates and incidence of ASD is significantly lower in randomized studies. This data further supports the need for comprehensive analysis of all available studies to gain a broad understanding of potential complications. The use of only prospective, randomized controlled trials may bias the literature and lead to large complications not being further addressed. The variables of most interest from all included studies are further discussed below.
Reoperation Rate
Overall, the combined rates of reoperation for any reason for TDA and ACDF were 5.6% and 7.8%, respectively (P=0.06). However, while many studies included in this systematic review reported significantly lower TDA secondary surgery rates1,19,21,30,41-43,60,65, many also reported lower rates in ACDF, or insignificant differences between the two groups16,20,23,27,33,43,53,55. This may be due to differences in follow-up times, patient inclusion criteria, or limited ACDF patient data for comparison to TDA.
Reoperation rates at the adjacent level were similar between patients with TDA and patients with ACDF (4.8% v. 5.8%, P=0.67) (Table 2). Several of the studies included in the present analysis reported significantly lower adjacent level surgeries for TDA patients, as compared to ACDF patients2,29,30,35,41,42,57. In contrast, others reported that there was no difference in adjacent level surgeries1,16,17,21,23,59. This suggested that the motion preserving quality of TDA may not reduce the need for adjacent level surgeries, as intended. However, the removal rate at the index level between TDA and ACDF was statistically significant (P=0.04). Further, the revision and supplemental fixation rates were also significantly different between ACDF and TDA, favoring TDA patients (Table 2). This indicated all additional surgical intervention categories should be compared and assessed when comparing overall outcome of TDA. Accordingly, TDA patients appeared to have an overall favorable reoperation outcome when compared to ACDF patients.
There was some question of validity for reoperation rates as a significant long-term efficacy metric. The decision to operate could be considered highly subjective and dependent on the surgeon. However, this point is often refuted using the fact that reoperation rate is a dichotomous variable that requires significant symptomatic signs to move forward with surgery33. To demonstrate the efficacy of reoperation as a metric more studies should be done outside of the context of FDA IDE approval trials to determine the influence of surgical bias.
Preservation of Motion
As expected, range of motion, both at the index level, and for the cervical spine as a whole, was larger for patients with TDA, when compared to fusion. As C5/C6 and C6/C7 made up over 80% of the data reported, the results of the present review may be more representative of those levels and range of motion at the preceding levels could have a different outcome. Intuitively, fusion surgeries restricted motion at the index level, while TDAs retained almost all pre-operative motions. The biomechanical and pathological implications of ROM are still largely unclear, but if it is a priority for the patient to regain full range of motion following surgery, TDA is clearly the better option.
Adjacent Segment Degeneration
There was a significant difference in the incidence of ASD for TDA patients and ACDF patients (26.2% v. 43.9%, P<0.001). This indicated that, as intended, disc arthroplasty appeared to reduce ASD, while fusions tended to increase stresses on adjacent levels. There were some inconsistencies among the included studies regarding the way in which ASD was quantified and reported. Some authors defined ASD as the need for surgical intervention, while others considered it an umbrella term for any postoperative new symptoms which developed at the adjacent level16,80. This demonstrated the need for more objective criteria for the evaluation and quantification of adjacent level disorders that develop postoperatively.
Heterotopic Ossification and Bone Adaptation
The overall incidence of HO of any grade was 43.89% for TDA, however the rate of motion-limiting HO (Grade 4) was much lower at 13.84%. This was consistent with findings reported by other investigators26,30,36,40. Although HO is a common complication of TDA, the impact that it has on clinical outcome is still largely unclear35. The present review indicated high rates of HO in studies with more than five years of clinical follow-up.
While the majority of the studies discussed heterotopic ossification, the abnormal growth of bone, postoperatively, very few reported the observation of osteolysis. Only one of the sixty studies reviewed reported that six patients displayed early signs of osteolysis resulting in a malalignment of the implant33. Further studies are needed in order to determine the prevalence and clinical ramifications of osteolysis in cervical TDA patients. At present, it is not clear if studies are overlooking bone loss or if similar observations are being reported using other umbrella terms81.
Clinical Outcomes
Overall patient satisfaction and functionality as assessed by the NDI Scores, VAS neck and/or arm pain scores, and SF-36 scores all significantly improved over baseline at the time of final follow-up for both TDA and ACDF, indicating that overall, both treatments were effective and patients were satisfied. All comparative studies with clinical outcome scores reported TDA as either significantly better than or non-inferior to ACDF1,2,15,17,18,21,25,29,30,35-38,40-42,44,47,48,50,55,62. Although difficult to quantify, the preservation of motion using TDA may allow the body to maintain a natural kinematic state after surgery. In contrast, fusion may place constraints on the spine, which could result in an overall lower clinical outcome rating for measures evaluating perceived health and functionality.
Limitations
There were several limitations in the present study. First, the only outcome data included for ACDF were studies that included ACDF patients as their control group. This may not be representative of general population of fusion patients, which may include patients that are not candidates for TDA surgeries. However, our study was focused on TDA performance, so the use of ACDF patients who were eligible for a TDA may be more appropriate. Additionally, while most studies reported similar categories of data, the way in which data was reported was not entirely consistent. For example, some authors reported overall reoperation rates, while others specified the location and extent of additional surgical procedures. Lack of cervical level-specific outcome in many of the studies is another potential weakness; however, more than 80% of the studies specified that levels treated were C5/C6 and C6/C7, the most widely indicated levels for TDA treatment. The majority of studies matched treated levels for comparison between ACDF and TDA patients; thus we can assume most ACDF surgeries were for C5/C6 or C6/C7, as well. Since we did not have the raw data from each study, reported means and standard deviations were used, with the inherent assumption that the general population is normally distributed.
Conclusion
The results of this study demonstrate the importance of including all possible studies and accounting for the potential of financial bias in reported outcomes. By reviewing all mid- to long-term data on cervical disc arthroplasty, this study provided a comprehensive overview of the performance of cervical disc arthroplasty. The results of this study suggest that TDA was successful in the general population at preserving motion, reducing adjacent segment degeneration, and improving overall quality of life, using standardized metrics for reporting.
Conflict of Interest
This study was partially supported by a research grant from OrthoFix, Plano, TX paid to the corresponding author’s institution.
References
- Burkus JK, Haid RW, Traynelis VC, et al. Long-term clinical and radiographic outcomes of cervical disc replacement with the Prestige disc: results from a prospective randomized controlled clinical trial. Journal of neurosurgery Spine. 2010; 13(3): 308-18. doi:10.3171/2010.3.SPINE09513
- Delamarter RB, Zigler J. Five-year reoperation rates, cervical total disc replacement versus fusion, results of a prospective randomized clinical trial. Spine (Phila Pa 1976). 2013; 38(9): 711-7. doi:10.1097/BRS.0b013e3182797592
- Goffin J, Geusens E, Vantomme N, et al. Long-term follow-up after interbody fusion of the cervical spine. Journal of spinal disorders & techniques. 2004; 17(2): 79-85. doi:10.1097/00024720-200404000-00001
- Chang K-E, Pham MH, Hsieh PC. Adjacent segment disease requiring reoperation in cervical total disc arthroplasty: A literature review and update. Journal of Clinical Neuroscience. 2017; 37: 20-24. doi:https://doi.org/10.1016/j.jocn.2016.10.047
- Kong L, Cao J, Wang L, et al. Prevalence of adjacent segment disease following cervical spine surgery: A PRISMA-compliant systematic review and meta-analysis. 2016; 95(27): e4171. doi:10.1097/md.0000000000004171
- Lehman R, Bevevino AJ, Brewer DD, et al. A systematic review of cervical artificial disc replacement wear characteristics and durability. Evidence-based spine-care journal. 2012; 3(S1): 31-8. doi:10.1055/s-0031-1298606
- Zhang Y, Liang C, Tao Y, et al. Cervical total disc replacement is superior to anterior cervical decompression and fusion: a meta-analysis of prospective randomized controlled trials. PloS one. 2015; 10(3): e0117826. doi:10.1371/journal.pone.0117826
- Mummaneni PV, Amin BY, Wu JC, et al. Cervical artificial disc replacement versus fusion in the cervical spine: a systematic review comparing long-term follow-up results from two FDA trials. Evidence-based spine-care journal. 2012; 3(S1): 59-66. doi:10.1055/s-0031-1298610
- Wang Q-l, Tu Z-m, Hu P, et al. Long-term Results Comparing Cervical Disc Arthroplasty to Anterior Cervical Discectomy and Fusion: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Orthopaedic surgery. 2020; 12(1): 16-30. doi:https://doi.org/10.1111/os.12585
- Wu TK, Liu H, Wang BY, et al. Minimum four-year subsequent surgery rates of cervical disc replacement versus fusion: A meta-analysis of prospective randomized clinical trials. Orthopaedics & traumatology, surgery & research : OTSR. 2017; 103(1): 45-51. doi:10.1016/j.otsr.2016.10.008
- Findlay C, Ayis S, Demetriades AK. Total disc replacement versus anterior cervical discectomy and fusion. The Bone & Joint Journal. 2018; 100-B(8): 991-1001. doi:10.1302/0301-620x.100b8.bjj-2018-0120.r1
- Nichol AD, Bailey M, Cooper DJ. Challenging issues in randomised controlled trials. Injury. 2010; 41 Suppl 1: S20-3. doi:10.1016/j.injury.2010.03.033
- Shamseer L, Moher D, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ : British Medical Journal. 2015; 349: g7647. doi:10.1136/bmj.g7647
- McAfee PC, Cunningham BW, Devine J, et al. Classification of heterotopic ossification (HO) in artificial disk replacement. Journal of spinal disorders & techniques. 2003; 16(4): 384-9. doi:10.1097/00024720-200308000-00010
- Cao FJ, Liu T, Xu YQ, et al. Comparison of Clinical and Radiographic Changes after Bryan Disc Arthroplasty versus ACDF: A 60-Month Follow-up on 120 Patients. World Journal of Neuroscience. 2015; 5: 40-48.
- Coric D. Prospective randomized study of cervical arthroplasty and anterior cervical discectomy and fusion with long-term follow-up: results in 74 patients from a single site. Journal of neurosurgery Spine. 2013; 18: 9.
- Coric D. Prospective, Randomized Multicenter Study of Cervical Arthroplasty Versus Anterior Cervical Discectomy and Fusion. JNS Spine. 2018; 28: 10.
- Gao X. A Comparison of Cervical Disc Arthroplasty and Anterior Cervical Discectomy and Fusion. World neurosurgery. 2019; 122: 7.
- Gornet MF, Lanman TH, Burkus JK, et al. Two-level cervical disc arthroplasty versus anterior cervical discectomy and fusion: 10-year outcomes of a prospective, randomized investigational device exemption clinical trial. Journal of neurosurgery Spine. 2019: 1-11. doi:10.3171/2019.4.spine19157
- Kumar C. Long-Term Comparison of Health Care Utilization and Reoperation Rates in Patients Undergoing Cervical Disc Arthroplasty and Anterior Cervical Discectomy and Fusion for Cervical Degenerative Disc Disease. World neurosurgery. 2020; 134: 11.
- Lanman TH. Long-term clinical and radiographic outcomes of the Prestige LP artificial cervical disc replacement at 2 levels: results from a prospective randomized controlled clinical trial. JNS Spine. 2017; 27(1): 13.
- Lei T, Liu Y, Wang H, et al. Clinical and radiological analysis of Bryan cervical disc arthroplasty: eight-year follow-up results compared with anterior cervical discectomy and fusion. Int Orthop. 2016; 40(6): 1197-203. doi:10.1007/s00264-015-3098-7
- MacDowall A, Skeppholm M, Lindhagen L, et al. Artificial disc replacement versus fusion in patients with cervical degenerative disc disease with radiculopathy: 5-year outcomes from the National Swedish Spine Register. Journal of neurosurgery Spine. 2018; 30(2): 159-167. doi:10.3171/2018.7.SPINE18657
- Malham GM, Parker RM, Ellis NJ, et al. Cervical artificial disc replacement with ProDisc-C: clinical and radiographic outcomes with long-term follow-up. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia. 2014; 21(6): 949-53. doi:10.1016/j.jocn.2013.09.013
- Mehren C. Clinical and radiological outcome at 10 years of follow-up after total cervical disc replacement. European Spine Journal. 2017; 26: 9.
- Nunley PD. Heterotopic Ossification After Cervical Total Disc Replacement at 7 Years—Prevalence, Progression, Clinical Implications, and Risk Factors. International Journal of Spine Surgery. 2018; 12(3): 10.
- Phillips FM. Long-term Outcomes of the US FDA IDE Prospective, Randomized Controlled Clinical Trial Comparing PCM Cervical Disc Arthroplasty With Anterior Cervical Discectomy and Fusion. 2015; 40(10): 10.
- Quan GMY. Eight-Year Clinical and Radiological Follow-Up of the Bryan Cervical Disc Arthroplasty. Spine. 2011; 36(8): 8.
- Radcliff K. Long-term Evaluation of Cervical Disc Arthroplasty with the Mobi-C© Cervical Disc: A Randomized, Prospective, Multicenter Clinical Trial with Seven-Year Follow-up. International Society for the Advancement of Spine Surgery. 2017; 11(4): 19.
- Radcliff K, Coric D, Albert T. Five-year clinical results of cervical total disc replacement compared with anterior discectomy and fusion for treatment of 2-level symptomatic degenerative disc disease: a prospective, randomized, controlled, multicenter investigational device exemption clinical trial. Journal of neurosurgery Spine. 2016; 25(2): 213-24. doi:10.3171/2015.12.SPINE15824
- Ryu WHA. Long-term kinematic analysis of cervical spine after single-level implantation of Bryan cervical disc prosthesis. The Spine Journal. 2013; 13: 7.
- Shang Z, Zhang Y, Zhang D, et al. Clinical and Radiological Analysis of Bryan Cervical Artificial Disc Replacement for "Skip" Multi-Segment Cervical Spondylosis: Long-Term Follow-Up Results. Med Sci Monit. 2017; 23: 5254-5263. doi:10.12659/msm.904863
- Skeppholm M. Higher reoperation rate following cervical disc replacement in a retrospective, long-term comparative study of 715 patients. European Spine Journal. 2017; 26: 7.
- Tian W, Yan K, Han X, et al. Comparison of the Clinical and Radiographic Results Between Cervical Artificial Disk Replacement and Anterior Cervical Fusion: A 6-Year Prospective Nonrandomized Comparative Study. Clinical spine surgery. 2017; 30(5): E578-E586. doi:10.1097/BSD.0000000000000206
- Vaccaro A, Beutler W, Peppelman W, et al. Long-Term Clinical Experience with Selectively Constrained SECURE-C Cervical Artificial Disc for 1-Level Cervical Disc Disease: Results from Seven-Year Follow-Up of a Prospective, Randomized, Controlled Investigational Device Exemption Clinical Trial. International journal of spine surgery. 2018; 12(3): 377-387. doi:10.14444/5044
- Zeng J, Liu H, Rong X, et al. Clinical and radiographic outcomes of cervical disc arthroplasty with Prestige-LP Disc: a minimum 6-year follow-up study. BMC musculoskeletal disorders. 2018; 19(1): 285. doi:10.1186/s12891-018-2201-9
- Aghayev E, Bärlocher C, Sgier F, et al. Five-year results of cervical disc prostheses in the SWISSspine registry. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2013; 22(8): 1723-30. doi:10.1007/s00586-013-2770-0
- Burkus JK, Traynelis VC, Haid RW, et al. Clinical and radiographic analysis of an artificial cervical disc: 7-year follow-up from the Prestige prospective randomized controlled clinical trial: Clinical article. Journal of neurosurgery Spine. 2014; 21(4): 516-28. doi:10.3171/2014.6.spine13996
- Guo H, Sheng J, Sheng WB, et al. An Eight-Year Follow-Up Study on the Treatment of Single-Level Cervical Spondylosis Through Intervertebral Disc Replacement and Anterior Cervical Decompression and Fusion. Orthopaedic surgery. 2020; 12(3): 717-726. doi:10.1111/os.12634
- Han X, He D, Zhang N, et al. Comparison of 10-year Outcomes of Bryan Cervical Disc Arthroplasty for Myelopathy and Radiculopathy. Orthopaedic surgery. 2019; 11(6): 1127-1134. doi:10.1111/os.12565
- Hisey MS, Zigler JE, Jackson R, et al. Prospective, Randomized Comparison of One-level Mobi-C Cervical Total Disc Replacement vs. Anterior Cervical Discectomy and Fusion: Results at 5-year Follow-up. International journal of spine surgery. 2016; 10: 10. doi:10.14444/3010
- Janssen M, Zigler J, Spivak J, et al. ProDisc-C Total Disc Replacement Versus Anterior Cervical Discectomy and Fusion for Single-Level Symptomatic Cervical Disc Disease: Seven-Year Follow-up of the Prospective Randomized U.S. Food and Drug Administration Investigational Device Exemption Study. The Journal of Bone & Joint Surgery. 2015; 97: 1738-1747. doi:10.2106/JBJS.N.01186
- Sasso WR, Smucker JD, Sasso MP, et al. Long-term Clinical Outcomes of Cervical Disc Arthroplasty: A Prospective, Randomized, Controlled Trial. Spine (Phila Pa 1976). 2017; 42(4): 209-216. doi:10.1097/brs.0000000000001746
- Song Q, He D, Han X, et al. Clinical and radiological outcomes of cervical disc arthroplasty: ten year follow-up study. Int Orthop. 2018; 42(10): 2389-2396. doi:10.1007/s00264-018-3947-2
- Walraevens J, Demaerel P, Suetens P, et al. Longitudinal prospective long-term radiographic follow-up after treatment of single-level cervical disk disease with the Bryan Cervical Disc. Neurosurgery. 2010; 67(3): 679-87. doi:10.1227/01.neu.0000377039.89725.f3
- Wang LN, Hu BW, Wang L, et al. Clinical and radiographic outcome of dynamic cervical implant (DCI) arthroplasty for degenerative cervical disc disease: a minimal five-year follow-up. BMC musculoskeletal disorders. 2018; 19(1): 101. doi:10.1186/s12891-018-2017-7
- Yang H, Lu X, Yuan W, et al. Artificial disk replacement in the treatment of degenerative cervical disk disorder: a 30-year follow-up study. Spine (Phila Pa 1976). 2014; 39(19): 1564-71. doi:10.1097/brs.0000000000000484
- Yang SD, Zhu YB, Yan SZ, et al. Anterior cervical discectomy and fusion surgery versus total disc replacement: A comparative study with minimum of 10-year follow-up. Scientific reports. 2017; 7(1): 16443. doi:10.1038/s41598-017-16670-1
- Zhao Y, Sun Y, Zhou F-F, et al. Cervical disc arthroplasty with ProDisc-C artificial disc: 5-year radiographic follow-up results. Chinese medical journal. 2013; 126: 3809-11. doi:10.3760/cma.j.issn.0366-6999.20131733
- Zhao YB, Sun Y, Chen ZQ, et al. Application of cervical arthroplasty with Bryan cervical disc: long-term X-ray and magnetic resonance imaging follow-up results. Chinese medical journal. 2010; 123(21): 2999-3002.
- Dejaegher J, Walraevens J, van Loon J, et al. 10-year follow-up after implantation of the Bryan Cervical Disc Prosthesis. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2017; 26(4): 1191-1198. doi:10.1007/s00586-016-4897-2
- Dufour T, Beaurain J, Huppert J, et al. Clinical and radiological evaluation of cervical disc arthroplasty with 5-year follow-up: a prospective study of 384 patients. European Spine Journal. 2019; 28(10): 2371-2379. doi:10.1007/s00586-019-06069-z
- Ghobrial GM, Lavelle WF, Florman JE, et al. Symptomatic Adjacent Level Disease Requiring Surgery: Analysis of 10-Year Results From a Prospective, Randomized, Clinical Trial Comparing Cervical Disc Arthroplasty to Anterior Cervical Fusion. Neurosurgery. 2019; 84(2): 347-354. doi:10.1093/neuros/nyy118
- Goffin J, van Loon J, Van Calenbergh F, et al. A clinical analysis of 4- and 6-year follow-up results after cervical disc replacement surgery using the Bryan Cervical Disc Prosthesis. Journal of neurosurgery Spine. 2010; 12(3): 261-9. doi:10.3171/2009.9.spine09129
- Gornet MF, Burkus JK, Shaffrey ME, et al. Cervical Disc Arthroplasty with Prestige LP Disc Versus Anterior Cervical Discectomy and Fusion: Seven-Year Outcomes. International journal of spine surgery. 2016; 10: 24. doi:10.14444/3024
- Hu X, Jiang M, Liu H, et al. Five-Year Trends in Center of Rotation After Single-Level Cervical Arthroplasty with the Prestige-LP Disc. World neurosurgery. 2019; 132: e941-e948. doi:10.1016/j.wneu.2019.07.042
- Jackson RJ, Davis RJ, Hoffman GA, et al. Subsequent surgery rates after cervical total disc replacement using a Mobi-C Cervical Disc Prosthesis versus anterior cervical discectomy and fusion: a prospective randomized clinical trial with 5-year follow-up. Journal of neurosurgery Spine. 2016; 24(5): 734-45. doi:10.3171/2015.8.spine15219
- Kim KS, Heo DH. Do Postoperative Biomechanical Changes Induce Heterotopic Ossification After Cervical Arthroplasty?: A 5-Year Follow-up Study. Clinical spine surgery. 2016; 29(6): E309-13. doi:10.1097/bsd.0000000000000054
- Lavelle WF, Riew KD, Levi AD, et al. Ten-year Outcomes of Cervical Disc Replacement With the BRYAN Cervical Disc: Results From a Prospective, Randomized, Controlled Clinical Trial. Spine (Phila Pa 1976). 2019; 44(9): 601-608. doi:10.1097/brs.0000000000002907
- Loumeau TP, Darden BV, Kesman TJ, et al. A RCT comparing 7-year clinical outcomes of one level symptomatic cervical disc disease (SCDD) following ProDisc-C total disc arthroplasty (TDA) versus anterior cervical discectomy and fusion (ACDF). European Spine Journal. 2016; 25: 2263-2270.
- Park JY, Kim KH, Kuh SU, et al. What are the associative factors of adjacent segment degeneration after anterior cervical spine surgery? Comparative study between anterior cervical fusion and arthroplasty with 5-year follow-up MRI and CT. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2013; 22(5): 1078-89. doi:10.1007/s00586-012-2613-4
- Pointillart V, Castelain JE, Coudert P, et al. Outcomes of the Bryan cervical disc replacement: fifteen year follow-up. Int Orthop. 2018; 42(4): 851-857. doi:10.1007/s00264-017-3745-2
- Sun Y, Zhao YB, Pan SF, et al. Comparison of adjacent segment degeneration five years after single level cervical fusion and cervical arthroplasty: a retrospective controlled study. Chinese medical journal. 2012; 125(22): 3939-41.
- Zhao Y, Zhang Y, Sun Y, et al. Application of Cervical Arthroplasty With Bryan Cervical Disc: 10-Year Follow-up Results in China. Spine. 2016.
- Zigler JE. ProDisc-C and Anterior Cervical Discectomy and Fusion as Surgical Treatment for Single-Level Cervical Symptomatic Degenerative Disc Disease. Spine. 2013; 38(3): 7.
- Cao S, Zhao Y, Sun Y, et al. Single-level Cervical Arthroplasty with Prodisc-C Vivo Artificial Disc: Five-year Follow-up Results From One Center. Spine (Phila Pa 1976). 2022; 47(2): 122-127. doi:10.1097/brs.0000000000004119
- Genitiempo M, Perna A, Santagada DA, et al. Single-level Bryan cervical disc arthroplasty: evaluation of radiological and clinical outcomes after 18 years of follow-up. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2020; 29(11): 2823-2830. doi:10.1007/s00586-020-06486-5
- Kim K, Hoffman G, Bae H, et al. Ten-Year Outcomes of 1- and 2-Level Cervical Disc Arthroplasty From the Mobi-C Investigational Device Exemption Clinical Trial. 2021; 88(3): 497-505. doi:10.1093/neuros/nyaa459
- Lobo J, Linhares D, Lopes JMM, et al. Results of Total Cervical Disc Replacement with a Minimum Follow-up of 10 Years. Revista brasileira de ortopedia. 2020; 55(2): 185-190. doi:10.1055/s-0039-3400526
- Nunley PD, Kerr EJ, Cavanaugh DA, et al. Adjacent Segment Pathology After Treatment With Cervical Disc Arthroplasty or Anterior Cervical Discectomy and Fusion, Part 2: Clinical Results at 7-Year Follow-Up. International journal of spine surgery. 2020; 14(3): 278-285. doi:10.14444/7037
- Nunley PD, Kerr EJ, Cavanaugh DA, et al. Adjacent Segment Pathology After Treatment With Cervical Disc Arthroplasty or Anterior Cervical Discectomy and Fusion, Part 1: Radiographic Results at 7-Year Follow-Up. International journal of spine surgery. 2020; 14(3): 269-277. doi:10.14444/7036
- Zhao Y, Zhou F, Sun Y, et al. Single-level cervical arthroplasty with ProDisc-C artificial disc: 10-year follow-up results in one centre. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2020; 29(11): 2670-2674. doi:10.1007/s00586-019-06110-1
- Zhou F, Li S, Zhao Y, et al. Quantitative analysis of the correlation between preoperative cervical degeneration and postoperative heterotopic ossification after cervical disc replacement: minimum 10-year follow-up data. Journal of neurosurgery Spine. 2020. doi:10.3171/2020.4.spine191303
- Barbagallo GM, Certo F, Visocchi M, et al. Double-level cervical total disc replacement for adjacent segment disease: is it a useful treatment? Description of late onset heterotopic ossification and review of the literature. European review for medical and pharmacological sciences. 2014; 18(1 Suppl): 15-23.
- Meng Y, Wang X, Zhao Z, et al. Intraoperative Anterior Migration of the Prestige-LP Cervical Disc Owing to an Inappropriate Implantation Sequence During Continuous 2-Level Artificial Cervical Disc Replacement: A Case Report with 8-Year Follow-Up. World neurosurgery. 2018; 116: 194-200. doi:10.1016/j.wneu.2018.05.093
- Zeng J. Clinical and radiographic outcomes of cervical disc arthroplasty with Prestige-LP Disc: a minimum 6-year follow-up study. 2018; 19(285): 7.
- Peinemann F, Tushabe DA, Kleijnen J. Using multiple types of studies in systematic reviews of health care interventions--a systematic review. PloS one. 2013; 8(12): e85035. doi:10.1371/journal.pone.0085035
- Reddy AK, Anderson JM, Gray HM, et al. Clinical Trial Registry Use in Orthopaedic Surgery Systematic Reviews. J Bone Joint Surg Am. 2021; 103(10): e41. doi:10.2106/jbjs.20.01743
- Dorey F, Grigoris P, Amstutz H. Making do without randomised trials. The Journal of bone and joint surgery British volume. 1994; 76(1) :1-3.
- Hilibrand AS, Robbins M. Adjacent segment degeneration and adjacent segment disease: the consequences of spinal fusion? The spine journal : official journal of the North American Spine Society. 2004; 4(6 Suppl): 190s-194s. doi:10.1016/j.spinee.2004.07.007
- Wahbeh JM, Park SH, Campbell P, et al. The lexicon for periprosthetic bone loss versus osteolysis after cervical disc arthroplasty: a systematic review. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2022. doi:10.1007/s00586-021-07092-9
Appendix
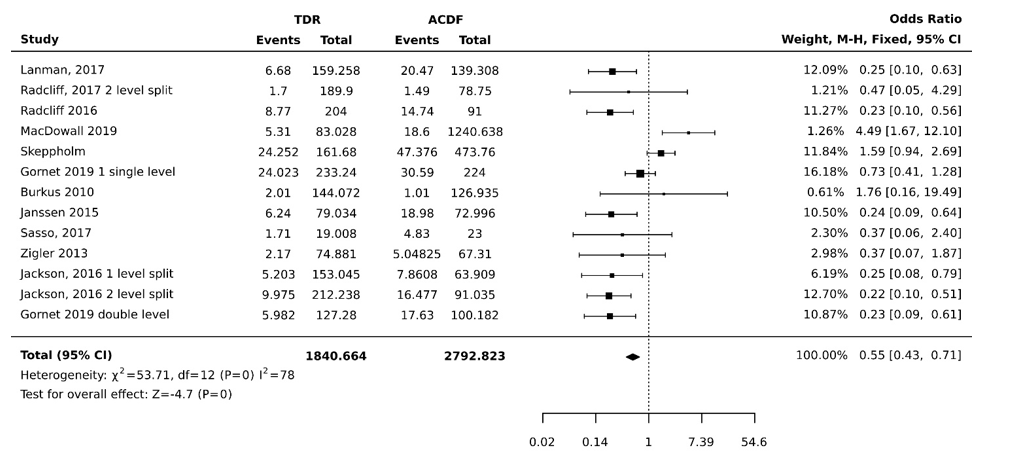
Figure 1: Index Level Reoperation rate statistical analysis for odds ratio and confidence intervals for studies comparing TDR patients and ACDF patients.
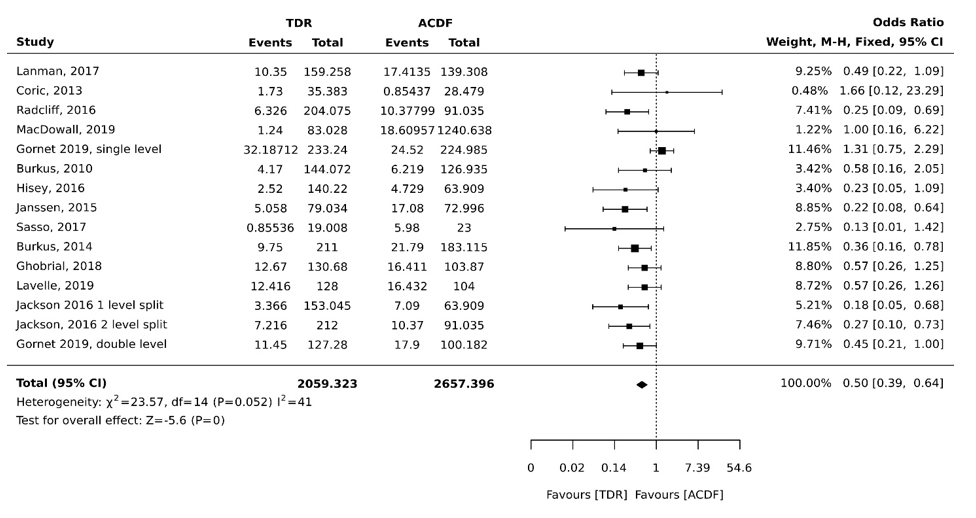
Figure 2: Adjacent Level Reoperation rate statistical analysis for odds ratio and confidence intervals for studies comparing TDR patients and ACDF patients.
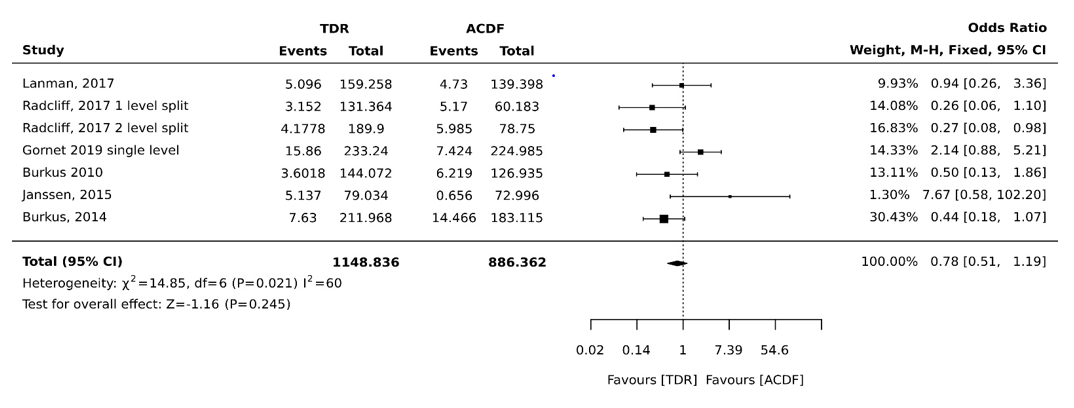
Figure 3: Removal rate statistical analysis for odds ratio and confidence intervals for studies comparing TDR patients and ACDF patients.
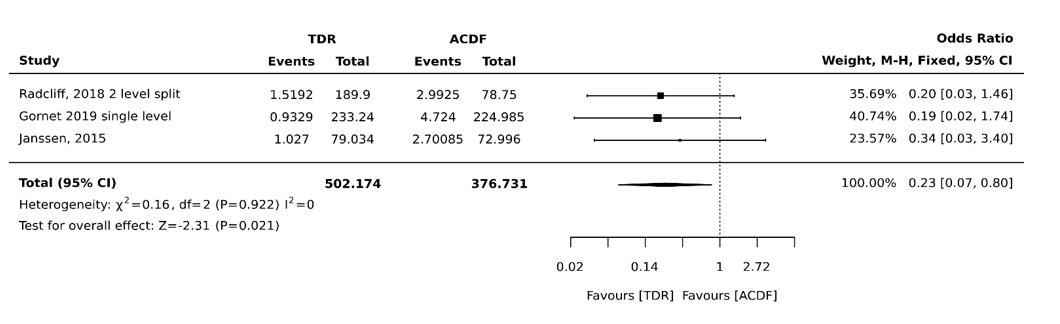
Figure 4: Revision rate statistical analysis for odds ratio and confidence intervals for studies comparing TDR patients and ACDF patients.
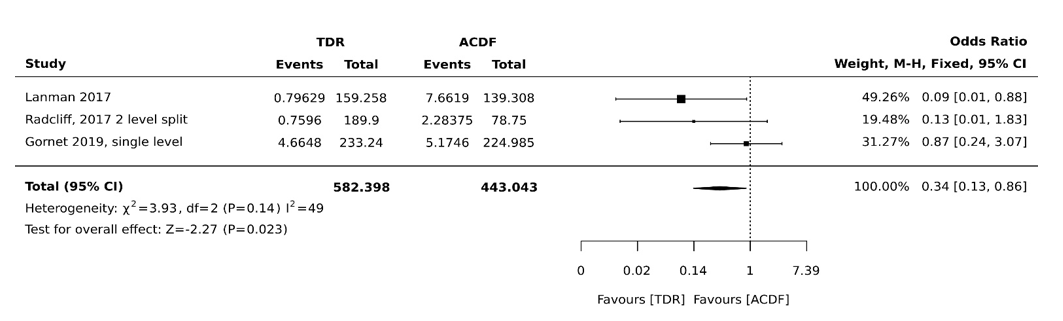
Figure 5: Supplemental fixation rate statistical analysis for odds ratio and confidence intervals for studies comparing TDR patients and ACDF patients