
Obstetric fracture of the femur during cesarean section in a preterm baby: A case report
Freddy Mertens Bombah¹*, Alphonse Ngalame², René Essomba³, Yannick Ekani Boukar², Enrique Zoa Nkoa4, Daniel Handy Eone4
1Department of Surgery and Specialty, Faculty of Medicine and Pharmaceutical Sciences, University of Douala, Cameroon
2Department of Gynecology and Obstetrics, Faculty of Health Sciences, University of Buea, Cameroon
3Department of Surgery and Specialty, Higher Institute of Medical Technology, University of Douala, Cameroon
4Department of Surgery and Specialty, Faculty of Medicine and Biomedical Sciences, University of Yaoundé I, Cameroon
Abstract
Introduction: Obstetric fractures or Birth fractures are rare events following childbirth. Although fracture of the femur is a relatively uncommon injury, it is the most common fracture of the lower extremity in the newborn. Since evolution of cesarean section rates in Africa, it is one of the most commonly practiced modes of delivery for breech. We described one case of fracture of the femur at cesarean section treated at Adlucem hospital in bonabéri-Douala (Cameroon).
Case report: A 2.1 kg male infant was delivered by lower segment cesarean section for breech presentation. Clinical and radiological examination showed shaft fracture of femur with good evolution.
Discussion: Fractures of the long bones are associated with cesarean section, breech delivery with assistance and low birth weight. Femoral fractures are the most associated long bones fracture with cesarean section.
Conclusion: The clinical and paraclinical diagnosis is simple and the management is mostly non-operative. It is important to explain to the parents and especially to the mother the benignity of the lesion.
Introduction
Obstetric fractures or Birth fractures are rare events following childbirth1. They can occur during vaginal or cesarean delivery1. Birth fractures almost always involve the clavicle, humerus, and femur2. Although fracture of the femur is a relatively uncommon injury, it is the most common fracture of the lower extremity in the newborn2,3. The majority of neonatal femoral fractures occur following vaginal breech delivery[nadas]. Since evolution of cesarean section rates in Africa, it is one of the most commonly practiced modes of delivery for breech4. One tends to think that birth femur fracture does not occur in these babies who are delivered by cesarean section. We therefore present this case and six other similar, previously reported cases to increase the awareness of this problem. It is also possible that many other cases may not have been reported in the literature2. We described one case of fracture of the femur at cesarean section treated at Adlucem hospital in bonabéri-Douala (Cameroon).
Case Report
A 26-year-old nondiabetic multigravida (Pregnancy 3 and childbirth 3) mother who was treated with quinine in the third trimester of pregnancy for Malaria. At the gestational age of 34 weeks, she had uterine contraction with signs of acute fetal distress. A 2.1 kg female infant was delivered by lower segment cesarean section for breech presentation. During cesarean section the obstetrician encountered difficulty in delivering the baby due to the engagement of fœtal breech. The baby cried immediately at birth. Apgar scores were 7 and 9 at 1 and 5 minutes, respectively. On the 1st day the examination revealed swelling in the left mid-thigh region and a click in the left femur. The left leg's mobility was very decreased compared with the right. The rest of the examination was unremarkable. Radiographic examination The X-ray of the left thigh revealed a femur fracture type 32-D/5.1 AO Pediatric Comprehensive Classification of Long-bone Fracture (PCCF) (Figure 1). After two days of stuck traction, hip spica cast (extends from the torso down to the foot) was applied, and the baby was discharged home. A follow-up radiograph at three weeks showed callus formation at the site of fracture and also a periosteal reaction at the site of fracture (Figure 2). A follow-up radiograph at 9 months showed good healing and the baby was doing well clinically. The neonatal course and 9-month follow-up with good recovery does not support the possibility of pathologic fracture, and no attempts were made to investigate further the cause of the fracture.
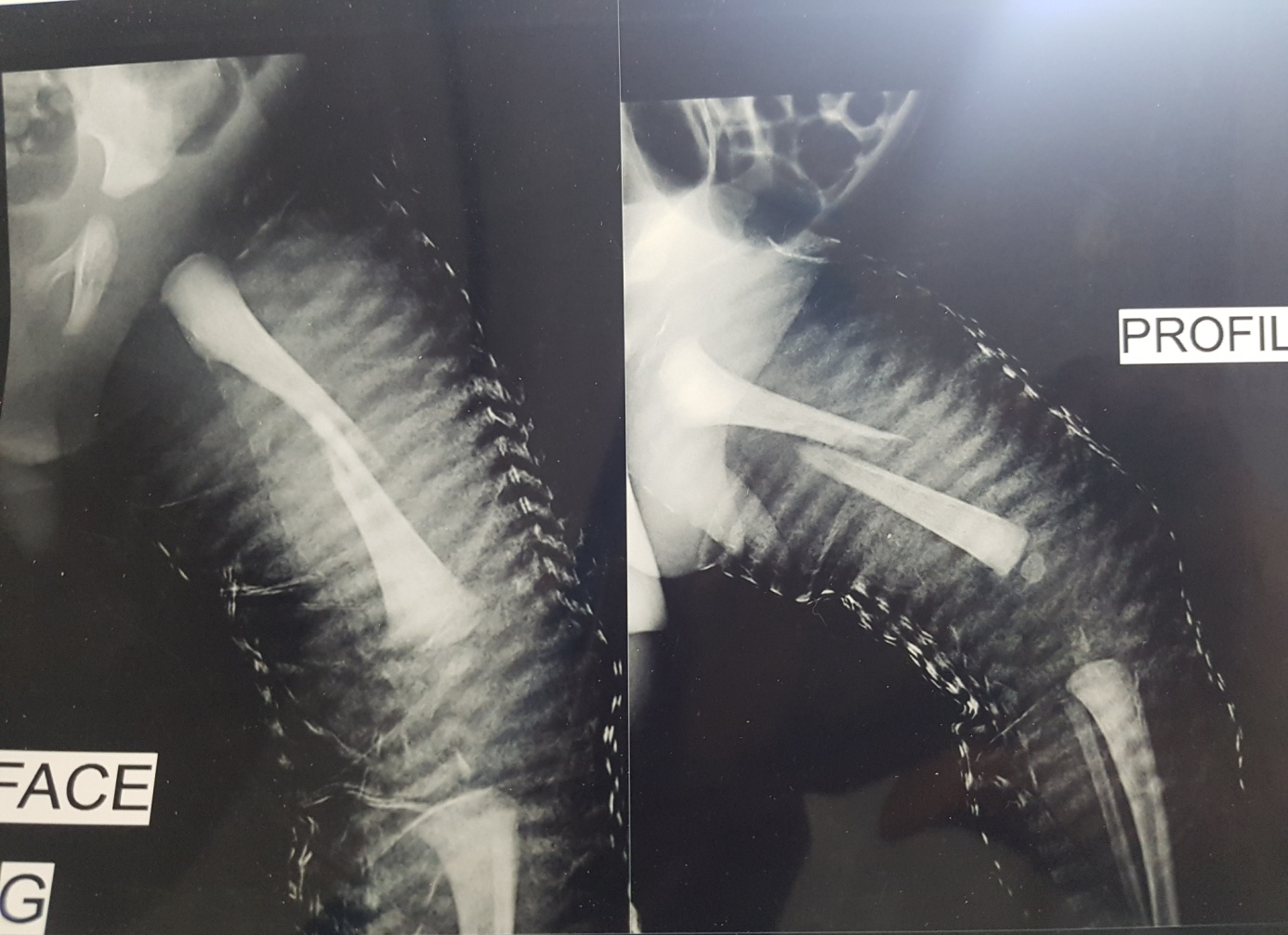
Figure 1: Femur fracture type 32-D/5.1 AO Pediatric Comprehensive Classification of Long-bone Fracture (PCCF)
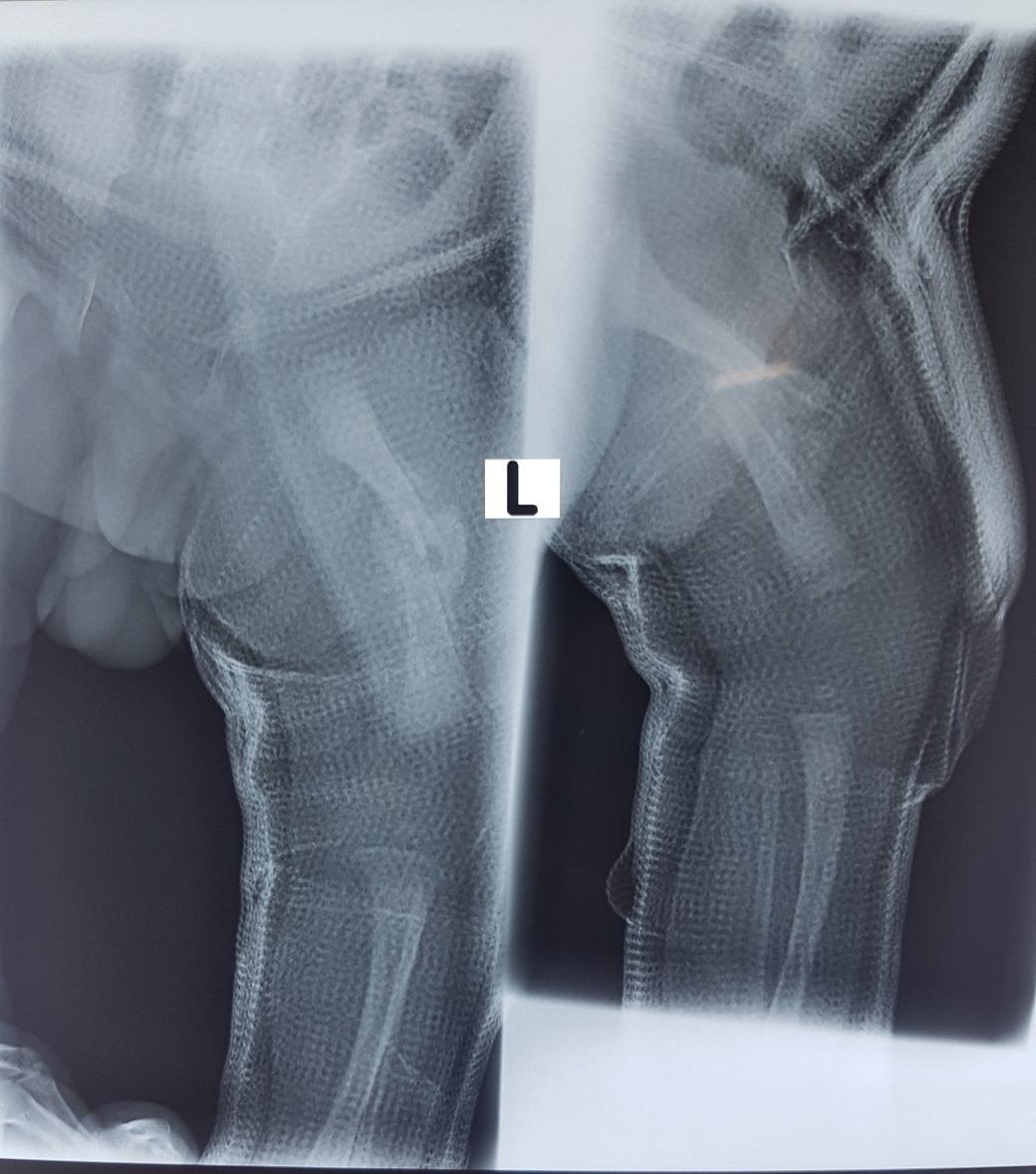
Figure 2: Showed callus formation at 3 weeks
Discussion
Obstetrical fracture can be divided into three (3) groups: depressed fractures of the skull, fractures of long bones and fractures of the clavicle5. There are many predisposing factors associated with these groups of obstetrical fractures5. Depressed skull fractures are associated with manoeuvres and the use of forceps during delivery5. Obstetrical fractures of long bones are rare. The reported incidence ranges from 0.028% to 0.054%5. Fractures of the long bones are associated with cesarean section, breech delivery with assistance and low birth weight5,6,7. Femoral fractures are the most associated long bones fracture with cesarean section5.
Long bone fractures do not pose diagnostic difficulties. A cracking sound can be heard in the delivery room. Deformation of the diaphyseal bone segment, pain during movement or a pseudo-paralytic attitude can be observed3. These fractures occur both in newborns of primiparous and multiparous mothers3. No study mentions prematurity in newborns like our case, but more the low birth weight5,6,7 or large babies with difficult delivery at cesarean section8,9. The paraclinical diagnosis makes it possible to make a diaphyseal or metaphyseal localization. In our case, the diagnosis of mid-diaphyseal fracture was made thanks to an X-ray, given the poverty of the family. According to Deschênes et al. standard radiography should be avoided whenever possible; ultrasound is the diagnostic tool of choice, completing the clinical examination before the age of 03 months3. It is important to explain to the parents and especially to the mother the benignity of the clinical and paraclinical lesion.
Diaphyseal femoral fractures are treated with cast immobilization without the need for precise alignment of bone fragments5,6,7. Newborns benefit from the extraordinary potential for skeletal remodeling at this age. Bonded traction can be used for femoral fractures1. It was used in our patient. There is no indication for surgical treatment1-10. Consolidation is constant and very quickly obtained1-10. In the event of a very unstable epiphyseal detachment fracture, surgical treatment by osteosynthesis may be necessary. Regular monitoring of the child until the end of growth is necessary. Complications included infection, malunion, nonunion are very rare. We have not found any in the literature. Bistoletti et al. reported 9.2% incidence of traumatic morbidity in infants delivered vaginally, but no incidence of traumatic morbidity in infants delivered by cesarean section10. Cesarean section does not reduce the traumatic morbidity in average-sized infants to zero2.
Conclusion
Femoral fractures at abdominal delivery are rare events. Most fractures occur in low birth weight and large babies with difficult delivery at cesarean section. The clinical and paraclinical diagnosis is simple and the management is mostly non-operative. It is important to explain to the parents and especially to the mother the benignity of the lesion.
Funding
None
Declaration of Competing Interest
None
References
- Blanc T, Bourgeois A, Deloin X, et al. 94 Fractures obstétricales: épidémiologie, présentation et prise en charge à propos de 70 cas. Revue de Chirurgie Orthopedique et Reparatrice de l'appareil moteur.2007; 93(7): 73.
- Vasa R, Kim MR. Fracture of the femur at cesarean section: case report and review of literature. American journal of perinatology.1990; 7(1): 46-48.
- Benhabiles A, Mahdjoub B. Traumatismes obstétricaux de l’appareil locomoteur: Où en sommes-nous? journal algérien de médecine. 2015; 23(2): 69-74.
- Cisse Cheikh T. Césariennes au Sénégal: couverture des besoins et qualité des services. Cahiers d'études et de recherches francophones/Santé.1998; 8(5): 369-377.
- Nadas S, Gudinchet F, Capasso P, et al. Predisposing factors in obstetrical fractures. Skeletal radiology. 1993; 22(3): 195-198.
- Hagglund G, Hansson LI, Wiberg G. Correction of deformity after femoral birth fracture: 16-year follow-up. Acta Orthop Scand. 1988; 59: 333-335.
- Kaplan M, Dollberg M, Wajntraub G, et al. Fractured long bones in a term infant delivered by cesarian section. Pediatr Radiol. 1987; 17: 256-257.
- Barnes AD, Van Geem TA. Fractured femur of the newborn at cesarean section. A case report. J Reprod Med. 1985; 30: 203-205.
- Alexander J, Gregg JEM, Quinn MW. Femoral fractures at cesarean section. Case reports. Br J Obstet Gynaecol. 1987; 94: 273.
- Bistoletti P, Nisell H, Palme C, et al. Term breech delivery, early and late complications. Acta Obstet Gynecol Scand. 1981; 60: 165-171.